Can Gum Disease Be Reversed? What a Periodontist Wants You to Know
Is Gum Disease Reversible?
Gingivitis (early-stage gum disease) is fully reversible with professional cleaning and improved oral hygiene. Periodontitis (advanced gum disease) is not reversible, but it can be successfully treated and managed to prevent further damage. The key factor is how early you seek treatment.
Understanding the Stages of Gum Disease
Gum disease progresses through distinct stages, each with different treatment outcomes:
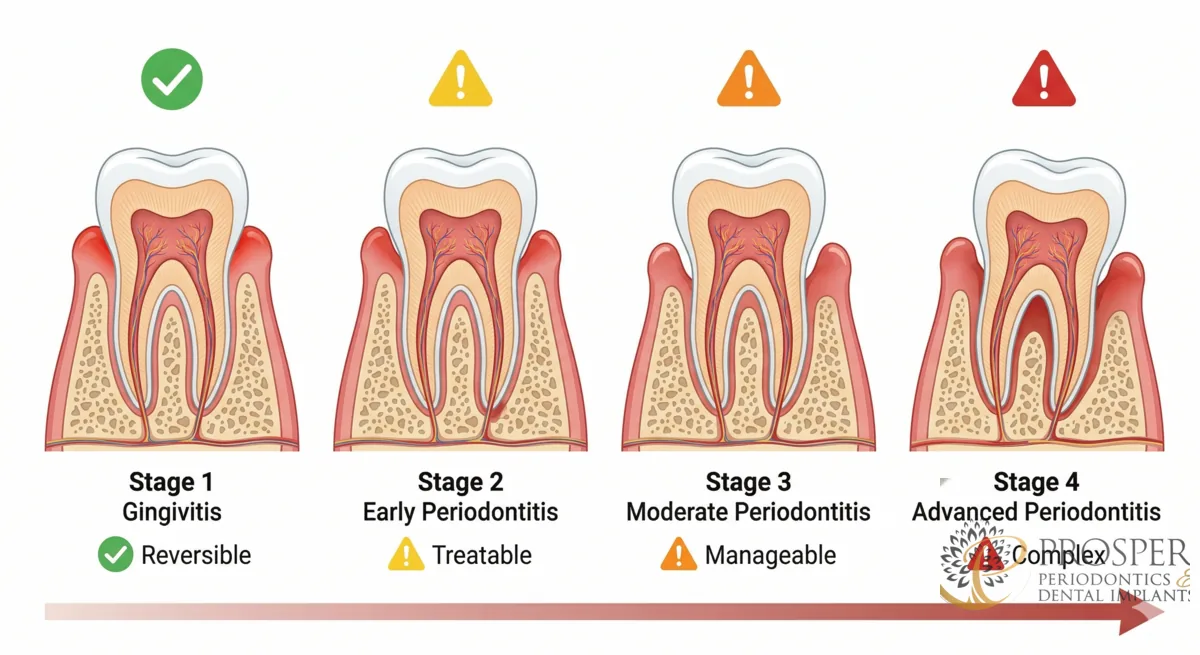
Stage 1: Gingivitis (Reversible)
Gingivitis is inflammation of the gums caused by plaque buildup. Symptoms include red, swollen gums that bleed when brushing. At this stage, no bone loss has occurred. Professional dental cleaning combined with proper brushing and flossing can completely reverse gingivitis.
Stage 2: Early Periodontitis (Treatable)
When gingivitis is left untreated, bacteria move below the gumline and begin to destroy the bone supporting your teeth. Pockets of 4 to 5mm form. The bone loss at this stage is permanent, but treatment can halt progression and prevent further damage.
Stage 3: Moderate Periodontitis (Treatable)
Pockets deepen to 5 to 7mm, and significant bone loss is visible on X-rays. Teeth may begin to shift or feel slightly loose. This stage requires active periodontal treatment such as LANAP laser therapy or traditional surgery.
Stage 4: Advanced Periodontitis (Treatable but Complex)
Severe bone loss, deep pockets (7mm+), tooth mobility, and potential tooth loss. Treatment is still possible but more complex, often involving multiple procedures including laser treatment, bone grafting, and potentially dental implants to replace lost teeth.
Can Lost Bone Be Regenerated?
Yes — LANAP is the only FDA-cleared laser treatment proven to regenerate lost periodontal bone. Research published in the Journal of Periodontology has shown that the PerioLase MVP-7 laser stimulates stem cells in the bone, facilitating true regeneration including new bone and new connective tissue attachment.
How to Prevent Gum Disease from Coming Back
- Brush twice daily with a soft-bristled or electric toothbrush
- Floss daily — no exceptions
- Schedule periodontal maintenance every 3 to 4 months
- Quit smoking — tobacco use is the #1 risk factor for gum disease progression
- Manage diabetes and other systemic conditions
Concerned about your gums? Call (972) 787-1122 or book an appointment with Dr. Parachuru at Prosper Periodontics.
What Is the Difference Between Reversing and Treating Gum Disease?
This distinction matters enormously and is one of the most misunderstood points in periodontal care. Reversing gum disease means the tissue returns to a fully healthy state with no permanent damage. Treating gum disease means stopping its progression, resolving active infection, and stabilizing the supporting structures – even though the bone and attachment already lost cannot be fully restored through treatment alone.
Gingivitis is fully reversible because no structural damage has occurred yet. The gum tissue is inflamed and infected, but the bone and connective tissue fibers attaching the gum to the tooth are still intact. A professional cleaning that removes the bacterial biofilm, combined with improved daily brushing and flossing, eliminates the source of inflammation. Within 2 to 4 weeks of consistent oral hygiene, the tissue returns to a healthy, firm, pale-pink state with no residual effects.
Once periodontitis begins, the damage is permanent but the disease is still manageable. Bone lost to periodontitis does not regenerate on its own. However, active treatment stops the infection, eliminates the destructive bacterial environment, and – in certain cases with LANAP laser therapy – can stimulate true bone regeneration in deficient areas. Patients who receive treatment and maintain a consistent periodontal maintenance schedule can keep their treated teeth for decades.
How Long Does It Take to Treat Each Stage of Gum Disease?
Treatment duration depends directly on how far the disease has advanced when you seek care. Here is a realistic timeline for each stage of treatment:
Gingivitis (4 to 8 weeks)
One or two professional cleanings combined with improved home care are typically sufficient to resolve gingivitis. Most patients see measurable improvement in gum firmness and reduction in bleeding within 2 to 4 weeks. A follow-up evaluation confirms resolution before returning to a standard 6-month recall schedule.
Early Periodontitis (2 to 4 months)
Scaling and root planing – deep cleaning below the gumline – is performed under local anesthesia, typically in 2 to 4 appointments covering quadrants of the mouth. A re-evaluation at 6 to 8 weeks post-treatment assesses pocket depth reduction and tissue response. Many early-stage patients achieve adequate control with non-surgical treatment alone and then transition to 3- to 4-month maintenance intervals.
Moderate to Advanced Periodontitis (4 to 12 months)
More advanced disease often requires either LANAP laser treatment or traditional periodontal surgery in addition to deep cleaning. LANAP is typically completed in 2 appointments covering the full mouth, with follow-up at 3, 6, and 12 months to monitor bone regeneration. Traditional osseous surgery may require 4 or more sessions. The entire active treatment phase, through stabilization, commonly spans 6 to 12 months before transitioning to ongoing maintenance.
What Does the Periodontal Maintenance Phase Actually Involve?
Periodontal maintenance is not the same as a regular dental cleaning, and this distinction is critical to preventing recurrence. After active periodontal treatment, the bacteria responsible for gum disease never fully disappear from the oral environment. They repopulate the pockets that were treated, and without regular professional disruption of that bacterial biofilm, the infection can re-establish itself within 3 to 4 months.
A periodontal maintenance appointment includes several components that a routine hygiene visit does not. These include:
- Full periodontal probing to measure pocket depths at every tooth and compare against baseline measurements
- Assessment of bone levels via updated X-rays at scheduled intervals
- Subgingival debridement – cleaning below the gumline in areas where pockets are still present
- Evaluation of gum recession and tissue health changes since the previous visit
- Reinforcement of home care techniques specific to the patient’s anatomy and risk profile
The 3-month interval is not arbitrary. Research demonstrates that pathogenic bacteria begin re-colonizing periodontal pockets approximately 9 to 11 weeks after professional debridement. The 3-month interval is designed to disrupt this recolonization before it reaches levels that cause renewed tissue damage. Patients who space appointments to 6 months post-treatment consistently show higher rates of disease recurrence than those who maintain the 3-month schedule.
Clinical Evidence
Patients placed on a 3-month professional maintenance program following active periodontal treatment showed dramatically lower rates of disease recurrence and tooth loss compared to patients receiving only annual recalls over a 6-year period. — Journal of Periodontology (Axelsson and Lindhe, 1981)
Can Lifestyle Changes Meaningfully Reverse Early Gum Disease at Home?
For gingivitis, the answer is a qualified yes – but only with the right technique and consistency. Most people who claim to brush twice daily are still missing the gumline, where the bacterial biofilm does the most damage. The toothbrush head needs to be angled at 45 degrees toward the gumline to clean the sulcus – the shallow groove where the gum meets the tooth. A soft-bristled brush used in small circular or vibrating motions for a full 2 minutes is more effective than a firm brush used aggressively.
Flossing is non-negotiable, not optional. No amount of brushing reaches the contact points between teeth, where roughly 40 percent of tooth surfaces reside. Floss or an interdental brush must curve around each tooth in a C-shape and slide 1 to 2 millimeters below the gumline to actually disrupt subgingival plaque. Water flossers are a useful adjunct, particularly for patients with dental implants, bridges, or braces, but they do not replace mechanical flossing for plaque disruption.
Beyond technique, several modifiable factors have strong evidence for either accelerating or slowing gum disease:
- Smoking cessation: Tobacco masks gum disease by constricting blood vessels and reducing bleeding – giving a false sense of health. Smokers who quit show rapid improvement in tissue response, though existing bone loss remains. Smoking cessation is the single most impactful lifestyle change a periodontal patient can make.
- Blood sugar management: For diabetic patients, improved glycemic control directly reduces the severity of gum disease and improves treatment outcomes.
- Anti-inflammatory diet: Diets high in omega-3 fatty acids, leafy greens, and low in refined carbohydrates have been associated with lower rates of periodontal disease in epidemiological studies.
- Stress reduction: Elevated cortisol impairs immune function and increases susceptibility to periodontal infection. Chronic stress is a documented independent risk factor for periodontitis progression.
Expert Insight
“I see patients every week who have been brushing and flossing faithfully for years but still have active gum disease. Technique matters as much as frequency. And for patients past the gingivitis stage, home care alone cannot treat the infection that is already established below the gumline. The bacteria living in a 6- or 7-millimeter pocket are in an anaerobic environment that no toothbrush or rinse can reach - that is where professional treatment becomes essential, not optional.”
— Dr. Parachuru, Periodontist
How Do You Know If Your Gum Disease Treatment Is Working?
There are clear, measurable indicators that periodontal treatment is succeeding. At each maintenance or re-evaluation appointment, your periodontist assesses these specific clinical markers:
Pocket Depth Reduction
Healthy pockets measure 1 to 3mm. After successful treatment, pockets that were 5 to 6mm should reduce to 4mm or less, and pockets that were 7mm or deeper should reduce by at least 2mm. If pockets are not reducing, the treatment approach needs to be reassessed.
Bleeding on Probing
Healthy gum tissue does not bleed when probed. Bleeding on probing (BOP) is recorded as a percentage of sites tested. After successful treatment, BOP should fall below 20 percent of sites. A BOP score above 30 percent is considered a reliable predictor of future disease progression if not addressed.
Bone Level Stability on X-rays
Serial X-rays taken at 12- to 18-month intervals allow your periodontist to confirm that bone levels are stable – neither continuing to decline nor (in the case of LANAP patients) showing the fill that indicates regeneration. Stable bone levels with no further loss is the primary long-term goal of periodontal treatment.
If you have completed periodontal treatment in the past but have not maintained your 3- to 4-month recall schedule, you may be at higher risk for recurrence than you realize. A re-evaluation appointment at Prosper Periodontics will show exactly where things stand. Learn more about the warning signs of active gum disease and explore how gum grafting can address recession that has developed as a result of periodontal disease. For patients with more advanced disease, review the comparison between LANAP and traditional surgery to understand your treatment options in full.
Clinical Evidence
Bleeding on probing exceeding 30 percent of sites is a statistically significant predictor of future attachment loss, supporting its use as a clinical threshold for treatment escalation in maintenance patients. — Journal of Clinical Periodontology (Lang and Tonetti, 2003)
Are There Patients for Whom Gum Disease Is Harder to Treat?
Yes – and being aware of these factors helps patients and clinicians set realistic expectations and design more targeted treatment plans. Several systemic and genetic factors make periodontal disease significantly more challenging to manage:
Genetic susceptibility plays a meaningful role. Research has identified specific interleukin-1 gene polymorphisms (IL-1A and IL-1B) that are associated with a 2 to 7 times greater risk of severe periodontitis and poorer response to non-surgical treatment. Genetic testing for periodontal susceptibility is available and can inform more aggressive treatment and maintenance planning in high-risk individuals.
Immunocompromised patients – including those on chemotherapy, long-term corticosteroids, or biologic medications for autoimmune conditions – have an impaired ability to control the bacterial challenge in periodontal pockets. These patients frequently require shorter maintenance intervals and may have limited response to standard treatment protocols.
Patients with osteoporosis experience accelerated alveolar bone loss when periodontitis is present, because the systemic bone density deficit compounds the localized bone destruction from the infection. Bisphosphonate medications used to treat osteoporosis also create specific risks that must be discussed with your periodontist before any surgical periodontal procedures or implant placement.
The good news is that even for the most complex patients, modern periodontal treatment offers meaningful options. LANAP laser treatment is particularly well-suited to medically complex patients because it involves no cutting or sutures, has minimal post-operative bleeding, and dramatically reduces the risk of complications compared to traditional surgery. A thorough review of your medical history is part of every treatment planning consultation at Prosper Periodontics.
Related Resources
Learn more about the services and topics discussed in this article:
- periodontal care
- LANAP laser treatment
- gum grafting
- warning signs of gum disease
- LANAP vs traditional surgery
Serving Prosper, TX and Surrounding Communities
Prosper Periodontics and Dental Implants proudly serves patients across North Dallas, including: periodontal care in Frisco, TX, laser gum treatment in Celina, TX. Schedule your appointment today.