Single Tooth Implant vs Bridge: Which Is Better?

When comparing a single tooth implant to a dental bridge, implants consistently outperform bridges in every long-term metric that matters: bone preservation, adjacent tooth health, longevity, and total cost of ownership over a lifetime. That said, bridges are not without merit for specific situations. This guide gives you the complete clinical picture so you can make an informed decision with your periodontist.
What Is the Difference Between a Single Tooth Implant and a Bridge?

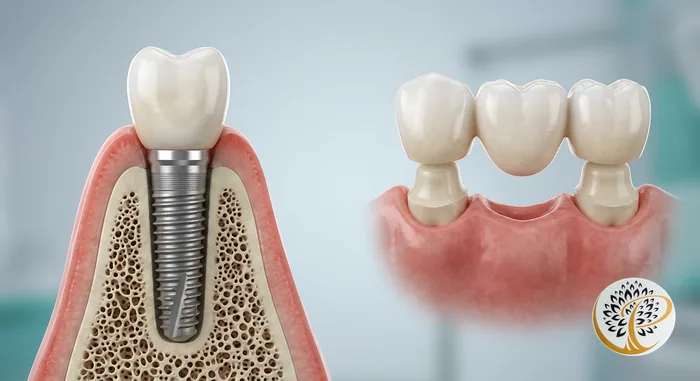
The core difference is what goes into the jaw. A dental implant replaces both the visible tooth crown and the underlying root structure using a titanium post that fuses to your bone. A dental bridge replaces only the visible crown, using the two teeth on either side of the gap as anchor (abutment) teeth – which must be ground down and permanently capped to hold the bridge in place.
That distinction – root vs. no root – drives almost every clinical difference between the two options. Bone requires stimulation from a root to maintain its density. An implant provides that stimulation. A bridge does not.
How Do They Compare Side by Side?
A direct comparison across the metrics that matter most to patients and clinicians reveals a clear pattern: implants win on biology, bridges win on upfront cost and speed.
| Factor | Single Tooth Implant | 3-Unit Dental Bridge |
|---|---|---|
| Upfront Cost | $3,000 to $5,500 | $2,000 to $5,000 |
| Typical Lifespan | 25 years to lifetime with maintenance | 10 to 15 years average |
| 30-Year Cost (estimated) | $4,000 to $6,000 (one-time) | $8,000 to $15,000 (replacements) |
| Adjacent Teeth Affected | None | Yes – both abutment teeth are permanently altered |
| Bone Preservation | Yes – stimulates bone | No – bone resorbs under the pontic |
| Treatment Timeline | 3 to 4 months (longer if bone graft needed) | 3 to 6 weeks |
| Cleaning Method | Brush and floss normally | Floss threader or water flosser required under bridge |
| Failure Risk to Neighboring Teeth | None | Decay risk at abutment margins; if one abutment fails, entire bridge fails |
| Feel and Function | Closest to natural tooth | Very good, but not independent |
| Insurance Coverage (typical) | Most plans cover both implant fixture and crown portion; some exclude implant fixture | More commonly covered under major restorative benefits |
| Candidacy Requirement | Adequate bone and healthy gums required | Healthy abutment teeth required |
Why Do Implants Preserve Bone and Bridges Do Not?
Bone is a living tissue that remodels in response to mechanical stress. When a tooth root transmits bite forces into the jawbone, the bone responds by maintaining and remodeling itself. This is the same biological principle behind why astronauts lose bone density in zero gravity – without load, bone resorbs.
When a tooth is extracted and not replaced with an implant, the bone at that site begins to shrink within the first year. Studies show an average bone loss of 25 percent in width during the first year, and roughly 4 millimeters of height over the following few years. A bridge replaces the crown but leaves the extraction site without a root substitute. Over a decade or more, this bone loss changes the profile of the jaw, creates a visible dip in the gum line beneath the bridge pontic, and can make future implant placement more difficult or require bone grafting.
An implant fixture, because it is anchored in bone and transmits bite forces just like a natural root, halts this process. The bone around a well-integrated implant maintains its density as long as the implant remains healthy.
Clinical Evidence
After tooth extraction, 50 percent of bone width is lost within 12 months, with the majority occurring in the first 3 months, highlighting the importance of root replacement for bone preservation. — Journal of Oral and Maxillofacial Surgery (Schropp L, Wenzel A, Kostopoulos L, Karring T, 2003)
What Is the Risk to Adjacent Teeth With a Bridge?
Placing a bridge requires permanently removing 60 to 70 percent of the enamel from the two healthy teeth on either side of the gap – teeth that may never have had a cavity in their life. Once crowned, those abutment teeth carry a higher lifetime risk of decay at the crown margin, pulp sensitivity, and eventual root canal treatment. Research published in the Journal of Dental Research found that approximately 30 percent of abutment teeth require root canal treatment within 10 years of bridge placement.
There is also a cascading failure risk. A bridge is a single unit connecting three teeth. If one abutment tooth fails – due to decay, root fracture, or periodontal bone loss – the entire bridge must be replaced. In contrast, an implant fails independently and has no effect on the teeth around it.
For patients with healthy adjacent teeth and adequate bone, a periodontist will almost universally recommend an implant over a bridge for this reason alone.
Clinical Evidence
Abutment teeth supporting fixed partial dentures (bridges) show a 30 percent incidence of pulp necrosis within 10 years, requiring root canal treatment in a significant proportion of cases. — Journal of Dental Research (Walton JN, 2002)
When Is a Dental Bridge the Better Choice?
Bridges have genuine clinical merit in specific circumstances, and a good periodontist will tell you when one makes more sense than an implant.
A bridge may be the better option when:
- Severe bone loss has occurred at the extraction site and the patient cannot or does not wish to undergo bone grafting before implant placement.
- The adjacent teeth already need crowns due to large existing restorations or structural damage. If you were going to crown those teeth anyway, a bridge can be an efficient solution.
- Timeline is the priority. A bridge can be completed in 3 to 6 weeks. If you need a solution quickly for a visible front tooth, a bridge delivers results faster.
- Medical contraindications for surgery exist, such as active chemotherapy, poorly controlled diabetes, or certain blood-thinning medication protocols that cannot be paused.
- Financial constraints make the lower upfront cost of a bridge necessary in the short term, with the understanding that replacement costs will be higher over time.
How Does Insurance Coverage Differ Between Implants and Bridges?
Dental insurance historically favors bridges over implants, though this gap is narrowing as implants become the clinical standard of care.
A traditional 3-unit bridge is categorized under “major restorative” benefits by most insurers and may be covered at 50 percent after your deductible, up to your annual maximum (typically $1,500 to $2,000). The bridge itself may cost $2,500 to $5,000, so insurance may reduce your out-of-pocket cost by $750 to $1,500.
For implants, many PPO plans now cover implant fixture, abutment and crown portion at 50-80 percent rate. Some plans have begun covering the full implant system as clinical guidelines have shifted. It is worth calling your insurer directly and asking whether they cover “endosseous dental implants” – the specific billing language matters.
Neither procedure typically resets your lifetime maximum, so timing matters if you have remaining annual benefits. Our team can help you review your coverage and maximize your insurance before starting treatment.
What Do Periodontists Look For When Recommending One Over the Other?
The clinical decision framework considers bone volume, adjacent tooth condition, patient health, timeline, and the patient’s long-term goals in that order.
Bone Assessment
A cone beam CT scan measures available bone at the proposed implant site. If there is adequate volume (minimum 10 mm height, 6 mm width), an implant is typically the first recommendation. If significant bone loss has occurred, the discussion shifts to whether bone grafting is viable and desired.
Adjacent Tooth Condition
If the teeth flanking the gap are healthy and untouched by significant restorations, preserving them is a strong argument for the implant. If they are already heavily restored or compromised, the argument against a bridge weakens.
Systemic Health and Lifestyle
Active smokers, patients with uncontrolled systemic disease, and patients on certain medications require additional evaluation. These factors may affect osseointegration success and tip the recommendation toward a bridge in some cases. Read our post on signs of gum disease for context on how periodontal health plays into this decision.
Patient Priorities
Some patients prioritize the fastest timeline. Others want to avoid surgery. A small number have religious or personal objections to titanium implants and prefer zirconia or non-implant solutions. These priorities are valid inputs into the clinical decision.
Expert Insight
“When I have a patient with a healthy adjacent tooth on each side of a gap and enough bone to work with, recommending a bridge would mean permanently damaging two healthy teeth to support one prosthetic. That trade-off almost never makes clinical sense. But I always walk through the full picture with the patient, because their priorities and health history matter.”
— Dr. Parachuru, Periodontist
How Do Implants and Bridges Differ in Maintenance?
An implant is maintained the same way you maintain a natural tooth: brushing twice daily and flossing. The implant crown sits at or slightly above the gum line and can be flossed exactly like a real tooth. Interdental brushes and water flossers add extra protection around the implant-gum interface.
A bridge requires cleaning the area beneath the pontic (the false middle tooth) where the bridge spans the gap. Food debris and plaque accumulate in this space and must be cleaned with a floss threader, superfloss, or water flosser. This is manageable but adds steps to daily hygiene compared to an implant or natural tooth.
Both options benefit from regular professional cleanings. Patients with implants should maintain periodontal maintenance appointments every 3 to 6 months to monitor peri-implant tissue health.
Frequently Asked Questions
Is getting a dental implant more painful than a bridge?
Implant placement requires a minor surgical procedure under local anesthesia, with sedation available. Most patients report less discomfort than they anticipated. Bridge preparation requires aggressive drilling on adjacent teeth, which can cause significant post-procedure sensitivity. Both involve some discomfort, but neither is typically described as severely painful when properly managed.
Can I get an implant years after having a tooth extracted?
Yes, though bone grafting may be required if significant resorption has occurred at the extraction site. A cone beam CT scan will confirm how much bone remains and whether grafting is needed before implant placement. Delays of several years are common and the majority of these cases can still be successfully treated.
Will my insurance pay for a dental implant in 2026?
Coverage varies widely. Many PPO plans now cover the implant fixture, abutment and crown portion at 50-80 percent. Ask your insurer specifically about “endosseous implants” under your major restorative benefit. Our front desk team can review your plan benefits before your consultation.
How long does a dental bridge actually last?
Clinical literature reports median bridge survival of 10 to 15 years, with many lasting longer when hygiene is excellent and adjacent teeth remain healthy. Some bridges fail early due to decay at the crown margins or abutment tooth fracture. Re-treatment at failure typically means another bridge (which shortens the adjacent teeth further) or converting to an implant at that point.
Does a dental implant look different from my other teeth?
No. The crown on an implant is custom-fabricated to match the shape, size, and shade of your surrounding teeth. In most cases, the result is indistinguishable from a natural tooth. Modern ceramic and zirconia crown materials allow precise color matching even for patients with naturally translucent enamel.
What if I am afraid of dental surgery?
We offer oral conscious sedation and IV sedation for patients with dental anxiety. Most implant placements take 45 to 90 minutes and patients who use sedation frequently report having little to no memory of the procedure. See our Sedation Dentistry page for available options and our patient guide to sedation.
Schedule Your Consultation
If you are weighing a dental implant against a bridge, the most important step is an in-person evaluation with a periodontist who can assess your bone, examine your adjacent teeth, and give you a clear recommendation based on your specific anatomy. Dr. Parachuru provides exactly this kind of patient-centered clinical guidance at Prosper Periodontics and Dental Implants. Call us at (972) 787-1122 or schedule your consultation online.
Related Resources
- Dental Implants – Full Service Overview
- Periodontal Care and Gum Health
- Dental Implant Cost in Prosper, TX
- Dental Implant Recovery Guide
- Signs of Gum Disease You Shouldn’t Ignore
- Your First Visit to a Periodontist: What to Expect
- Sedation Dentistry Options
Serving Prosper, TX and Surrounding Communities
We provide dental implant consultations and periodontal care for patients throughout North Texas, including those coming from Frisco and Celina. Located at 2300 E Prosper Trail Suite #20, Prosper, TX 75078, with easy access from US-380 and the Dallas North Tollway.