Bone Grafting for Dental Implants: Types and Recovery

For roughly one in three implant candidates, the conversation about implants starts with a separate conversation about bone. Years of missing teeth, periodontal disease, or trauma can leave the jaw without enough volume or density to anchor an implant securely, and bone grafting is the procedure that rebuilds that foundation. The good news is that grafting protocols are well-studied, the success rate is high, and the materials available today let the periodontist match the technique to the defect rather than the other way around. This guide walks through the four main graft material types, the most common surgical scenarios, the healing timeline, and the cost expectations. Dr. Praveen Parachuru plans bone grafting cases at Prosper Periodontics using 3D CBCT imaging and the protocols he learned during his periodontics certificate at the University of Minnesota.
Why Do So Many Implant Patients Need Bone Grafting?
Once a tooth is lost, the surrounding alveolar bone begins to resorb almost immediately, losing 25 percent of its volume in the first year and continuing to shrink over time without the mechanical stimulation that natural tooth roots provide. The result is a ridge that often does not have enough width or height to support an implant.
There are four common pathways that bring patients to the bone grafting conversation. The first is delayed implant placement after extraction, where months or years between losing the tooth and considering replacement let the ridge collapse. The second is periodontal disease, where chronic infection has already destroyed bone before the tooth was even removed. The third is trauma, including fractures and avulsion injuries. The fourth is anatomy, where the maxillary sinus naturally sits low above the upper back teeth and limits the vertical bone available for an implant.
The diagnostic step that determines whether grafting is needed is a 3D CBCT scan, which measures bone width, height, and density at every potential implant site with millimeter-level precision. A panoramic 2D X-ray cannot reliably show this. Dr. Parachuru uses CBCT planning at every implant consultation, which means the recommendation about whether grafting is needed is based on actual measurements rather than estimation.
Studies suggest that 30 to 40 percent of implant cases involve some form of bone augmentation, with the percentage higher in posterior maxillary cases and lower in anterior mandibular cases. Our dental implants service page covers the broader implant pathway.
What Are the Four Main Types of Bone Graft Material?

Bone graft materials fall into four categories: autograft (your own bone), allograft (processed human donor bone), xenograft (processed bovine bone), and alloplast (synthetic bone substitutes). Each has a profile of advantages, trade-offs, and best-use scenarios.
Autograft is bone harvested from the patient’s own body, typically from the chin, ramus of the lower jaw, or in larger cases the hip. It is considered the gold standard biologically because it contains the patient’s own living cells, growth factors, and bone matrix proteins. The trade-off is the need for a second surgical site and the additional recovery that creates. Autograft is most often selected for larger or more challenging defects where the biological activity matters most.
Allograft is processed human donor bone from tissue banks that follow strict screening, sterilization, and processing protocols. It provides an excellent scaffold for the patient’s own bone to grow into and avoids the second surgical site that autograft requires. Allograft is one of the most widely used materials in modern implant dentistry and has decades of published outcome data.
Xenograft is processed bovine (cow) bone, most commonly from the brand Bio-Oss, that has been treated to remove all organic material and leave only the mineral scaffold. It resorbs slowly, which makes it useful when long-term volume preservation is the goal, particularly in sinus lift and ridge augmentation cases. Alloplast is fully synthetic, made from materials like beta-tricalcium phosphate or hydroxyapatite. It avoids any human or animal source concerns and works well in defined defects, though it does not carry the biological activity of autograft.
Most modern grafting cases use a combination, often allograft mixed with xenograft, with a resorbable membrane placed over the graft to keep soft tissue from invading the space during healing. Dr. Parachuru selects materials based on defect size, location, healing biology, and patient preference.
What Is a Sinus Lift and When Is It Needed?
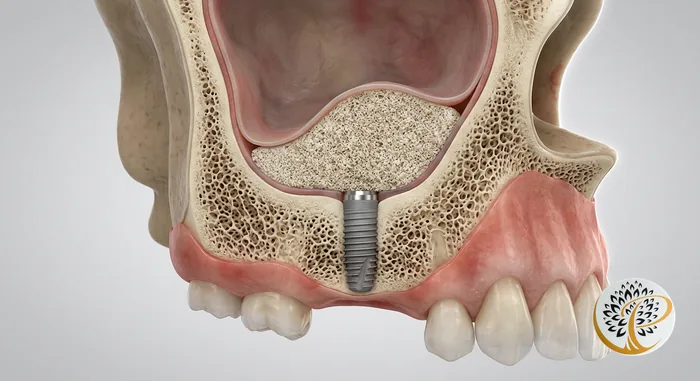
A sinus lift, also called sinus augmentation, is a specialized bone grafting procedure that adds bone to the upper posterior jaw by gently elevating the floor of the maxillary sinus and placing graft material in the created space. It is one of the most common grafting procedures because the maxillary sinus naturally limits available bone in that area.
The maxillary sinus is the air-filled space above the upper back teeth, separated from the mouth by a thin layer of bone and a sinus membrane. When upper molars are lost, the sinus tends to expand downward over time, sometimes leaving only 2 to 4 millimeters of bone where 8 to 10 millimeters are needed to anchor an implant. A sinus lift restores that vertical dimension by carefully elevating the membrane and placing graft material in the resulting void.
There are two surgical approaches. The lateral window technique is used when significant vertical augmentation is needed. A small access window is created in the side of the upper jaw, the membrane is elevated, and graft material is placed. Healing time before implants can be placed is typically 6 to 9 months. The crestal or osteotome technique is a less invasive option used when only a small amount of additional bone is needed (1 to 4 millimeters), and the lift can sometimes be performed at the same time the implant is placed.
Sinus lift success rates are high in published literature, with implant survival in grafted sinuses comparable to implant survival in native bone over long-term follow-up. The procedure is most often performed under local anesthesia with optional sedation, with a recovery profile similar to other grafting surgeries. Patients are advised to avoid blowing the nose forcefully, sneezing with mouth closed, and air travel for the first 1 to 2 weeks.
What Is Socket Preservation and Why Is It Important?
Socket preservation, also called ridge preservation, is a graft procedure performed at the time a tooth is extracted to preserve the bone volume of the empty socket and reduce the ridge collapse that otherwise begins immediately. It is the simplest and most preventive form of bone grafting.
When a tooth is extracted without socket preservation, the empty socket fills in with a blood clot that converts to soft tissue and then to bone over several months. During this process, the ridge typically loses 40 to 60 percent of its width and 20 percent of its height in the first year. That loss often determines whether a future implant will need additional grafting later.
Socket preservation is straightforward. After the tooth is removed, the periodontist places graft material into the socket and covers it with a resorbable membrane and sutures. Healing takes 3 to 5 months before the site is ready for an implant. The patient experiences minimal additional discomfort beyond the extraction itself, and the long-term ridge volume is substantially better preserved.
The decision point at extraction is whether you eventually want to replace the tooth with an implant, a bridge, or nothing. If implant replacement is on the table, even as a future possibility, socket preservation is almost always worth it. The cost of socket preservation at the time of extraction is significantly lower than the cost of corrective grafting later, and the outcome is more predictable.
What Is Ridge Augmentation and When Is It Done?
Ridge augmentation is a larger grafting procedure that rebuilds bone width or height in a ridge that has already collapsed, often from years of tooth loss, periodontal disease, or trauma. It is performed when a 3D scan shows the existing bone volume cannot anchor an implant safely.
There are two augmentation directions. Horizontal augmentation adds width to a knife-edge ridge that is too narrow for an implant. Techniques include particulate grafts contained by membranes, block grafts harvested from the chin or ramus, and ridge-splitting procedures where the existing ridge is gently widened and grafted from within. Vertical augmentation adds height and is technically more demanding because the body resists growing bone vertically more than horizontally. Techniques include guided bone regeneration with membranes and titanium mesh and, in select cases, distraction osteogenesis.
Healing after ridge augmentation typically takes 6 to 9 months before the implant can be placed. In larger cases, the implant is placed in a second surgical procedure once the augmented ridge has matured. In smaller cases, simultaneous augmentation and implant placement are sometimes possible. The decision depends on the size of the defect, the stability the implant can achieve at placement, and the morphology of the ridge.
Patient expectations matter here. Augmentation extends the total treatment timeline, often adding 6 to 12 months to the overall implant journey. The trade-off is an implant that has the bone foundation it needs to last, which our dental implant lifespan guide explores in more detail.
What Does Bone Graft Recovery Look Like?
Recovery from a bone graft procedure is generally less intense than patients expect: mild-to-moderate discomfort for 3 to 5 days, a soft-food diet for 1 to 2 weeks, and a longer behind-the-scenes healing period of 3 to 9 months while the graft integrates with the surrounding bone. Most patients return to work within 1 to 3 days.
The first week is the symptomatic phase. Swelling peaks at day 2 to 3, then subsides over the following week. Cold compresses on the first day reduce swelling. Pain is typically managed with prescription medication for the first day or two and over-the-counter ibuprofen or acetaminophen after that. A prescribed antimicrobial rinse replaces brushing at the surgical site for the first one to two weeks.
The diet matters. Soft, lukewarm foods only for the first week. No straws (the suction can disturb the graft and clot), no smoking, no alcohol, and no vigorous rinsing or spitting. Sneezing through an open mouth is recommended after a sinus lift to avoid pressure changes that could disturb the elevated membrane. Sutures are typically removed at 7 to 14 days.
The longer healing period is invisible from the outside. From month 2 through month 9 depending on the procedure, the graft material is gradually replaced by the patient’s own bone in a process called creeping substitution. By the time the implant is placed, the graft has matured into bone that integrates with the implant just like native bone. Our dental implant recovery guide covers what comes next.
How Much Does Bone Grafting Cost?
Bone grafting costs in the Prosper, TX area typically range from $400 to $1,200 for a single-site socket preservation, $1,500 to $3,500 for a sinus lift, and $2,500 to $5,000 or more for larger ridge augmentation cases. Costs vary with the size of the defect, the type of graft material, the use of a membrane, and whether sedation is included.
Insurance coverage for bone grafting in implant cases is mixed. Medical insurance sometimes covers grafting after trauma or in cases tied to a covered medical procedure. Dental insurance coverage varies by plan, with some plans covering a portion of the procedure when there is a documented diagnosis. Many implant cases require the patient to budget for some out-of-pocket grafting cost, even when they have decent coverage.
Pre-authorization with your insurance carrier before the procedure provides a written coverage estimate, which helps with planning. Our team handles pre-authorization and insurance verification on every case, and we provide a written treatment plan with itemized costs before any surgical commitment. Cherry Financing is available to spread costs over time. For the broader implant cost picture, see our dental implant cost guide for Prosper, TX.
The honest takeaway is that bone grafting is often a necessary investment in the success of the implant rather than an optional add-on. An implant placed in inadequate bone has a higher long-term failure rate, and the corrective cost of replacing a failed implant is substantially higher than the upfront cost of grafting. Our are dental implants worth it guide walks through the long-term value math.
Ready to Build the Foundation for Your Implant?
If you have been told you do not have enough bone for an implant, or if you are early in the implant conversation and want to understand what your specific case will require, the next step is a consultation with 3D CBCT imaging and a written treatment plan. Dr. Parachuru completed his periodontics certificate at the University of Minnesota with a PhD in Immunology, which means implant candidates at Prosper Periodontics are evaluated by a specialist who understands both the mechanical and biological factors that drive long-term implant success. We see patients from Prosper, Frisco, McKinney, Celina, and Aubrey at our office at 2300 E Prosper Trail Suite #20.
To schedule, call (972) 787-1122 or request a consultation online. Learn more about our protocols on the dental implants service page, explore the specialized procedures we offer, and review pricing on the dental implant cost guide for Prosper, TX. McKinney-area patients can read the dental implants in McKinney page.