All-on-4 Failure Rate: What the Research Really Shows

Patients researching All-on-4 inevitably land on horror-story forums, defensive marketing pages, and a wide spread of failure-rate numbers that range from “almost never fails” to “thousands of patients have problems.” The truth lives in the peer-reviewed literature, where two decades of long-term data make a more useful conversation possible. This guide walks through what the published studies actually show about implant failure, prosthesis complications, the risk factors that drive bad outcomes, and the questions to ask any provider before committing. Dr. Praveen Parachuru places All-on-4 cases at Prosper Periodontics using the same protocols studied in the original Malo Clinic research.
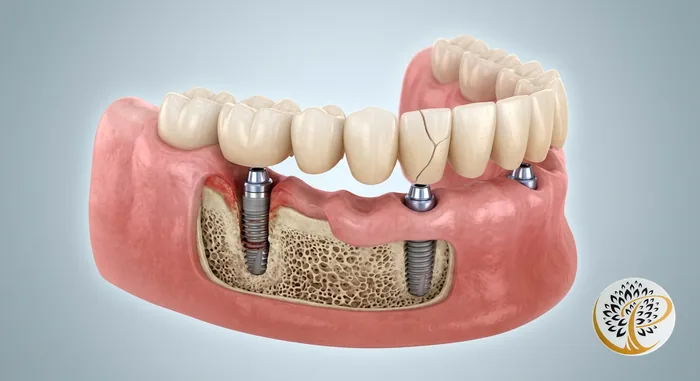
What Is the Actual All-on-4 Failure Rate?
Across long-term peer-reviewed studies, All-on-4 implant survival ranges from roughly 94 to 98 percent at ten years, which means the implant failure rate sits in the 2 to 6 percent range over a decade. That is the headline number, and it is consistent across multiple independent research groups.
The original Malo Clinic ten-year follow-up data, published across several papers between 2011 and 2019, reported cumulative implant survival of 94.8 to 98 percent depending on jaw and subgroup. Subsequent systematic reviews in journals like BMC Oral Health, Clinical Oral Implants Research, and the International Journal of Oral and Maxillofacial Implants have largely confirmed these ranges across diverse patient populations and surgical teams.
The numbers can be cut a few ways. Implant survival (the implant remaining in the jaw) sits at the higher end of the range. Implant success (the stricter definition that adds healthy bone levels and no inflammation) sits a few percentage points lower. Prosthesis survival is also slightly lower than implant survival, because the prosthesis can chip, screws can loosen, and wear accumulates over years.
Two patterns are worth noting. Mandibular cases outperform maxillary cases by one to three percentage points because lower jaw bone is denser. Cases placed by specialist periodontists and oral surgeons outperform cases placed by general dentists in comparative studies. The number that does not appear in serious clinical research is anything close to a “high failure rate.” Patients who arrive with that impression usually picked it up from forums where individual cases get amplified out of statistical context.
What Are the Different Types of All-on-4 Failure?
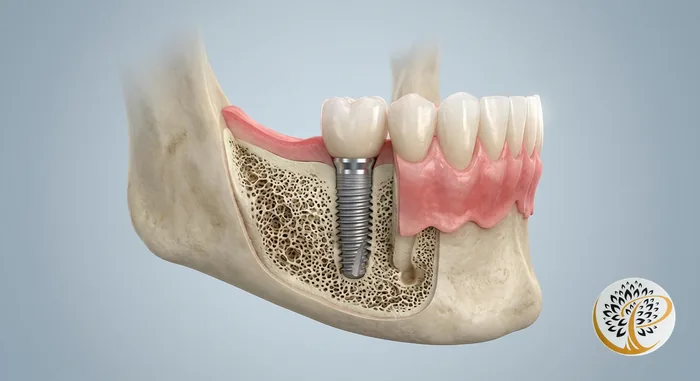
All-on-4 complications fall into three distinct categories: early implant failure, late implant failure, and prosthesis-level complications. Conflating them is the most common source of confusion in failure-rate conversations. Each has its own causes, timing, and resolution.
Early implant failure happens in the first three to six months when the implant does not osseointegrate. Reported rates are 2 to 5 percent at one year. The mechanisms are biological: the bone fails to fuse to the implant due to micro-motion during healing, contamination at placement, compromised host healing, or insufficient primary stability. The standard response is removal of the failed implant, a three-to-six-month healing window, and re-placement at the same or a modified site. Outcomes after re-placement are good.
Late implant failure happens months or years after successful integration. Reported rates are 5 to 10 percent over a ten-year window. The mechanism is almost always peri-implantitis, an inflammatory and infectious process that destroys supporting bone. Risk factors are smoking, poor home hygiene, missed maintenance visits, and a history of severe periodontitis. Caught early, peri-implantitis is treatable with non-surgical or surgical decontamination. Caught late, it can require implant removal.
Prosthesis-level complications are technically not implant failures and are managed as routine maintenance. They include screw loosening (5 to 25 percent over five years), porcelain or acrylic chipping (5 to 15 percent), prosthesis fracture (1 to 5 percent), and bite-surface wear. None threatens the underlying implants, and all are repairable in one or two appointments. They show up in horror-story forums because patients sometimes confuse a chipped tooth or loose screw with implant failure when the implant itself is solidly integrated.
Which Risk Factors Drive the Bad-Outcome End of the Curve?
Five risk factors disproportionately drive the difference between the 2 percent failure rate at the top of the range and the 6 percent rate at the bottom: smoking, uncontrolled diabetes, untreated periodontitis at placement, untreated bruxism, and skipped maintenance. Patients can modify all five.
Smoking is the largest single modifiable risk factor in the implant literature. Active smokers face implant failure rates two to three times higher than non-smokers. Nicotine restricts blood flow to healing tissue, reduces osseointegration completeness, and increases late peri-implantitis risk. Quitting before surgery and staying off nicotine through the healing period substantially closes the gap with non-smokers. Vaping carries similar risk and should be treated the same way.
Uncontrolled diabetes (HbA1c above 8.0 to 8.5 percent) impairs healing, alters bone metabolism, and increases infection risk. Diabetic patients with HbA1c under 7 percent have outcomes comparable to non-diabetic patients. Dr. Parachuru coordinates with the patient’s primary care physician or endocrinologist to confirm metabolic control before scheduling surgery.
Untreated periodontitis at placement raises long-term peri-implantitis risk because patients with active gum infection at the surgical sites carry that bacterial environment forward. The protocol at Prosper Periodontics is to treat active periodontal disease and confirm tissue stability before proceeding. This is not a delay; it is the foundation that separates favorable long-term outcomes from compromised ones.
Untreated bruxism generates biting forces that can exceed 250 pounds per square inch and accelerates prosthesis wear and screw loosening. A custom nightguard fabricated after the final prosthesis is placed addresses most of this risk. Skipped maintenance is the quietest risk factor and one of the most preventable. Patients who attend six-month professional maintenance and follow the home-care routine sit at the favorable end of the survival range. Patients who skip maintenance for years sit closer to the unfavorable end. Our broader dental implants worth-it analysis walks through how maintenance shapes long-term value.
Why Do Specialist Periodontist Outcomes Outperform General Dentist Outcomes?
Multiple comparative studies show that implants placed by specialist periodontists and oral surgeons achieve survival rates one to three percentage points higher than implants placed by general dentists, with the gap widening for complex full-arch cases like All-on-4. The drivers are training, case volume, and biology.
Periodontists complete a three-year specialty residency after dental school, focused on the bone, gum tissue, and implant biology that determine implant outcomes. Oral surgeons follow a similar specialty path. General dentists may complete weekend or week-long implant continuing education, which provides exposure but does not replicate the depth of specialist training. The difference shows up in case selection, surgical technique, and management of complications when they occur.
Case volume matters because surgical skill is a function of repetition. Specialists who place implants weekly maintain a level of mechanical and judgment-based skill that cannot be matched by occasional placement. The All-on-4 protocol in particular involves angled posterior implants placed with millimeter-level precision near the maxillary sinus and the inferior alveolar nerve. The margin for error is small.
Bone biology and tissue management are the third leg. Periodontists treat periodontitis and peri-implantitis as their primary clinical work, which informs placement decisions, soft-tissue technique, prosthesis interface design, and the bone graft or sinus considerations that arise in 20 to 30 percent of cases. The patient takeaway is to confirm the credentials of the provider doing the surgery and ask how many All-on-4 cases they handle annually.
What Should You Ask a Provider Before Committing?
Five questions reliably separate a thorough All-on-4 practice from a marketing-led one: Who places the implants? How are cases planned? What is the maintenance program? What does the warranty cover? And how are complications handled?
The first question is who places the implants. The answer should be a periodontist or oral surgeon with documented specialty training. If the answer is a general dentist who completed continuing education, that is a meaningful data point that does not automatically rule out the practice but changes the risk profile of the case.
The second is how cases are planned. The answer should include 3D CBCT imaging, digital surgical planning software, and a guided-surgery protocol. Practices that place All-on-4 from a 2D panoramic radiograph alone are working with substantially less information than the standard of care supports.
The third is the maintenance program. The answer should include scheduled six-month maintenance with implant-specific instrumentation, an annual prosthesis-removal cleaning, and a clear plan for what is included in the case price versus billed separately. Practices without a defined maintenance protocol are missing the single most important predictor of long-term success.
The fourth is the warranty. Most reputable implant systems carry manufacturer warranties on the implant itself, often for life, while the practice typically warrants placement and prosthesis for one to five years. Warranties that require continued participation in the maintenance program are reasonable and indicate that the practice understands what drives long-term outcomes.
The fifth is how complications are handled. The answer should be specific. What is the re-placement protocol if an implant fails to integrate, and is it included in the original case fee? How quickly can the patient be seen for a loose screw? What is the peri-implantitis treatment pathway? Specific answers indicate the practice has handled these scenarios. Vague answers are a flag. A bonus question for cautious patients is annual case volume. Fifty or more full-arch cases per year reflects depth of experience.
What Happens If Your All-on-4 Does Fail?
The honest answer is that failure is manageable. Early implant failure is corrected by replacing the affected implant after a healing period, late failure is treated with peri-implantitis therapy or implant replacement, and prosthesis complications are repaired in one or two visits. No failure mode in All-on-4 is catastrophic in the way conventional denture wearers sometimes imagine.
If a single implant fails to integrate in the first six months, the standard pathway is removal, a three-to-six-month healing window, and re-placement at the same or a slightly modified site. The other three implants typically continue to support the prosthesis during this period. Re-placement outcomes are good because the underlying biology that supports the original three implants generally also supports a re-do.
If peri-implantitis is identified at a routine maintenance visit, the response depends on severity. Mild cases are treated non-surgically with deep instrumentation and antimicrobial therapy. Moderate cases may require surgical access to clean the implant surface and sometimes regenerative grafting. Severe cases that have lost substantial bone may require implant removal and replacement. The earlier peri-implantitis is caught, the simpler the treatment, which is precisely why scheduled maintenance matters.
Prosthesis chips or fractures are usually repaired in one or two appointments. Modern milled zirconia prostheses are durable, but no material is unbreakable, and patients with repeated fracture usually have undiagnosed bruxism that resolves with a nightguard. A loose retentive screw is a thirty-minute visit: the prosthesis is removed, the screw is retorqued or replaced, and the prosthesis is reseated.
Studies suggest that patients who experience a complication and follow the recommended treatment pathway typically end up with a functional outcome comparable to patients who never had a complication. For the broader picture of long-term success across implant types, our dental implant lifespan guide covers the data.
How Do You Maximize Your Odds of a Good Outcome?
The patients who land in the favorable end of the survival range share five behaviors: they choose a specialist provider, they treat active periodontal disease before placement, they quit smoking, they wear their nightguard, and they attend every six-month maintenance visit. All five are within the patient’s control.
Choosing the right provider is the highest-leverage decision. The specialist-versus-general-dentist gap in the literature is real, and it is the one factor locked in at the start of the case. The other four behaviors can be adjusted along the way.
Treating active periodontal disease before placement is a question of timing. The responsible protocol is to address infection at the implant sites first and confirm tissue stability before placing implants. Patients who push to skip this step often pay for it years later in elevated peri-implantitis risk. The delay is typically six to twelve weeks. The benefit is decades of better tissue health.
Quitting smoking before surgery is the largest single modifiable risk reduction available. Six weeks of nicotine cessation before placement and through the integration period meaningfully closes the gap with non-smokers. Wearing the nightguard is the simplest of the five and has the highest compliance gap. Patients who use it consistently see substantially fewer prosthesis-level complications.
Attending every six-month maintenance visit is the closing behavior that holds the others in place. The visit is where peri-implant tissue is monitored, screw torque is checked, the prosthesis is professionally cleaned, and small issues are caught before they become large ones. The honest summary is that All-on-4 has a modest failure rate that becomes a very small failure rate when patients and providers do their respective jobs.
Ready to Restore Your Smile?
If you have been weighing All-on-4 and want a candid conversation about the realistic risk profile for your specific anatomy and health history, the next step is a consultation with 3D imaging, a periodontal evaluation, and a transparent discussion of what your individual outcome curve looks like. Dr. Parachuru completed his periodontics certificate at the University of Minnesota alongside a PhD in Immunology, which means All-on-4 candidates at Prosper Periodontics are evaluated by a specialist who understands both the surgical mechanics and the biology that drives long-term success. We see patients from Prosper, Frisco, McKinney, Celina, and Aubrey at our office at 2300 E Prosper Trail Suite #20.
To schedule, call (972) 787-1122 or request a consultation online. Learn more about our protocol on the All-on-4 service page, compare your options on our All-on-4 vs dentures guide, and review pricing on the dental implant cost guide for Prosper, TX. Celina-area patients can also review the All-on-4 in Celina page.