LANAP Success Rate: Clinical Evidence and Patient Outcomes

When patients ask whether LANAP actually works, they are asking two different questions at the same time. The first is whether the published clinical research supports the regenerative claims. The second is what real-world outcomes look like in their own mouth, with their own anatomy and risk profile. Both questions deserve a precise answer rather than marketing copy. This guide walks through the histological foundation of LANAP, the long-term clinical follow-up data, the typical pocket depth and attachment gain figures, and the honest comparison to traditional flap surgery. Dr. Praveen Parachuru performs LANAP at Prosper Periodontics using the certified protocol that the published evidence is built on.
What Does the Histological Evidence Actually Show About LANAP?
The Yukna et al. 2007 human histology study is the foundational evidence behind LANAP’s regenerative claim, and it remains the only published human histological evidence demonstrating new cementum, new periodontal ligament, and new alveolar bone formation following any laser-based periodontal therapy.
The study, published in the International Journal of Periodontics and Restorative Dentistry, examined teeth scheduled for extraction in patients with chronic periodontitis. The investigators treated one side of selected teeth with the LANAP protocol and the contralateral side with scaling and root planing alone. Three months later, the teeth were extracted as part of unrelated treatment plans, and the tissues were sectioned and examined histologically. The LANAP-treated sites showed new cementum deposition on previously diseased root surfaces, new periodontal ligament fibers inserting into that cementum, and new alveolar bone formation. The SRP-treated sites showed long junctional epithelium, which is the standard repair pattern in most periodontal therapy.
This distinction is the regulatory and clinical foundation for LANAP. The FDA 510(k) clearance for periodontal regeneration relies specifically on histological evidence of new attachment, not on indirect surrogates like radiographic bone fill. The Yukna study supplied that evidence. No other laser-based periodontal protocol has produced equivalent published human histology, which is why other dental lasers do not carry the same regenerative clearance.
It is worth being measured about what histology can and cannot prove. The 2007 study examined a relatively small number of treated sites. Subsequent histological work and longer-term clinical studies have supported the original findings, but evidence indicates that the magnitude of regeneration varies between patients and between defect types. Histology shows that regeneration is biologically possible with LANAP. It does not promise that every site in every patient will regenerate to the same degree.
What Pocket Depth Reductions Are Typical After LANAP?
Across multiple published studies, LANAP treatment is associated with average pocket depth reductions of two to four millimeters at the six-month re-evaluation, with the larger reductions concentrated in pockets that were initially deepest.
Pocket depth is the simplest periodontal outcome measure to track and the one most patients understand intuitively. A healthy pocket is one to three millimeters deep. Active periodontitis typically presents with pockets in the four-to-six millimeter range for moderate disease, and seven to nine millimeters or more for advanced disease. Pocket reduction is the operational goal of any periodontal therapy because deeper pockets harbor more bacteria, are harder to clean at home, and progress faster if left untreated.
The published LANAP literature is consistent on the typical pattern. A pocket that was six millimeters before treatment commonly measures three or four millimeters at the six-month follow-up. A pocket that was eight or nine millimeters often reduces to four or five millimeters. The reductions come from two mechanisms working together: actual reattachment of the gum to the tooth (the regenerative component) and tightening of inflamed tissue against the root as the inflammation resolves. Both mechanisms count in the clinical measurement. Patients who follow through with maintenance generally see these reductions hold over the years that follow.
Bleeding on probing is the other simple outcome measure. Bleeding sites indicate active inflammation. Studies suggest that LANAP reduces bleeding-on-probing scores by fifty to seventy percent at the six-month re-evaluation. That reduction is a strong predictor of disease stability over longer follow-up.
What Do the Five- and Ten-Year Follow-Up Studies Show?
Long-term clinical data on LANAP is more limited than for traditional surgery because LANAP is a younger protocol, but the available five-year and ten-year follow-up studies show stable pocket depth reductions and attachment levels in patients who maintain their professional cleaning schedule.
Traditional periodontal surgery has decades of long-term outcome data because it has been the standard of care for fifty years. LANAP cleared the FDA in 2004, which means the longest follow-up windows currently in the published literature run to roughly fifteen years. The studies that exist are encouraging. Patients followed for five years post-LANAP show maintained pocket depth reductions, sustained attachment gain, and tooth retention rates comparable to or slightly favoring LANAP relative to historical surgical comparators.
A few caveats are worth naming. Long-term outcomes in any periodontal therapy depend heavily on patient compliance with maintenance, smoking status, and management of other risk factors. Studies that select for compliant patients report better numbers than population-level data. The honest interpretation is that LANAP can deliver durable outcomes when paired with a maintenance program, and it can underperform when patients do not return for follow-up.
The other useful framing is tooth retention. Periodontitis is fundamentally a tooth-loss disease over decades. Studies that follow patients across multiple years and track which teeth are still in the mouth tend to favor any active periodontal therapy over no treatment. LANAP performs comparably to traditional surgery on this measure when both are paired with consistent maintenance. For broader context on what is and is not reversible in periodontal disease, our companion post on whether gum disease can be reversed walks through the biology.
How Does the Success Rate Compare to Traditional Flap Surgery?
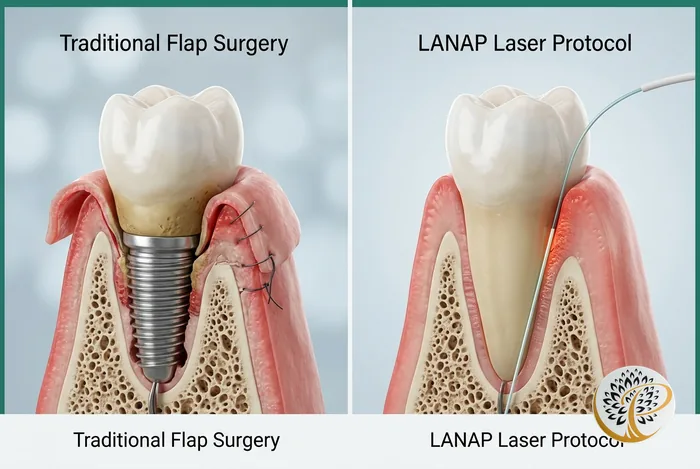
Comparative studies between LANAP and traditional osseous surgery show that pocket depth reductions and attachment gains are clinically comparable, while LANAP delivers those outcomes with markedly less recession, faster recovery, and a different long-term tissue architecture.
It is tempting to look for a single number that says LANAP is X percent better or worse than traditional surgery. The honest answer is that the two procedures heal differently, and a single comparison number obscures more than it reveals. Both produce clinically meaningful pocket reduction. Both reduce bleeding on probing. Both can stabilize active periodontitis. Where they differ is in the underlying tissue response.
Traditional osseous surgery resolves pockets primarily by repositioning the gumline at a lower level. The pocket depth measurement after surgery is shallower because the soft tissue starts at a more apical position. This is mechanically effective but produces visible recession at treated sites. The post-surgical tissue heals by repair (long junctional epithelium) rather than regeneration in most cases.
LANAP resolves pockets by reducing inflammation, allowing tissue tightening, and supporting regeneration of the attachment apparatus. The gumline does not retreat the same way it does after flap surgery. The post-treatment tissue, in published histological work, includes regenerated cementum, ligament, and bone at successful sites. Aesthetic outcomes favor LANAP, particularly in the front of the mouth where recession is most visible.
The honest comparison is captured in detail in our LANAP vs traditional gum surgery guide, which walks through the procedural differences side by side.
Why Does Provider Training Affect LANAP Outcomes So Much?
LANAP outcomes vary meaningfully by provider, and the most important predictor of a successful case is whether the doctor has completed the official LANAP certification training and uses the PerioLase MVP-7 with the standardized protocol.
LANAP is not just a laser. It is a defined protocol with specific laser settings at each step, a specific sequence of pocket measurement, laser passes, root debridement, and bite adjustment, and a defined post-operative maintenance schedule. The certification training is offered by the Institute for Advanced Laser Dentistry, which is the body authorized by Millennium Dental Technologies (the manufacturer of the PerioLase MVP-7) to certify operators. Dr. Parachuru completed this certification, which is the minimum credential required for any practice claiming to offer LANAP rather than a generic laser gum treatment.
You will sometimes encounter practices marketing “laser gum surgery” or “laser periodontal therapy” without being LANAP-certified or owning the PerioLase MVP-7 specifically. The treatment they are providing may use a diode or other laser for some bacterial reduction, which has clinical value, but it is not the LANAP protocol and does not carry the regenerative clearance. The distinction matters for patients trying to compare options.
The case-volume question is also relevant. Periodontists who perform LANAP routinely as part of their weekly practice maintain a level of mechanical and judgment-based skill that occasional operators do not. When you are evaluating a provider, it is reasonable to ask how long they have been LANAP-certified, what the PerioLase model is in their office, and roughly how many LANAP cases they treat in a typical month.
How Do Patient Behaviors Influence Long-Term Success Rates?
Five behaviors disproportionately separate the favorable end of the LANAP outcome distribution from the unfavorable end: smoking status, attendance at maintenance visits, home oral hygiene quality, control of systemic conditions like diabetes, and management of bruxism.
Smoking is the single largest modifiable risk factor in periodontology. Active smokers experience reduced LANAP outcomes the same way they experience reduced outcomes after traditional surgery, after dental implant placement, and after periodontal grafting. Nicotine restricts blood flow to gum tissue, impairs the wound-healing response that drives regeneration, and increases bacterial colonization of treated sites. Patients who quit at least six weeks before treatment and stay off nicotine through the healing window meaningfully close the gap with non-smokers. Vaping carries similar risks and should be treated the same way.
Maintenance attendance is the quietest predictor of long-term success. Periodontal maintenance every three to four months for the first year or two, transitioning to six-month intervals as tissue stability is confirmed, is the protocol that supports the durability of treatment. Patients who attend every visit on schedule sit at the top of the outcome distribution. Patients who skip years of maintenance lose ground that even successful initial treatment cannot make up.
Home hygiene quality matters because the day-to-day biofilm management between professional visits is where most disease activity is decided. Brushing technique, interdental cleaning with floss or interdental brushes, and consistent use of a soft brush head matter more than the specific products used. Antimicrobial rinses have a role in some patients but do not substitute for mechanical cleaning.
Systemic conditions feed back into periodontal outcomes. Diabetic patients with reasonable glucose control achieve LANAP results comparable to non-diabetic patients. Diabetics with HbA1c above eight percent should expect slower healing and potentially lower regeneration. The bidirectional relationship between gum disease and systemic health is the topic of our companion guide on the link between gum disease, heart disease, and diabetes. Untreated bruxism puts mechanical stress on healing tissue and undermines outcomes regardless of how the case starts.
What Should You Realistically Expect at Your Six-Month Re-Evaluation?
At the six-month re-evaluation visit, expect re-measurement of every pocket that was treated, a comparison to your baseline numbers, an assessment of bleeding on probing, and a candid conversation about whether additional therapy is needed at any specific sites.
The six-month visit is the operational assessment of whether LANAP worked. It is not a marketing visit. It is a clinical re-evaluation that quantifies what changed. Most pockets that started at five to seven millimeters typically measure three to five millimeters at this visit. Pockets that started at eight or nine millimeters often measure four to six millimeters, with deeper sites continuing to mature for several more months as the regenerative response completes.
A small percentage of treated sites do not respond as expected. The reasons range from anatomical (a furcation that the laser could not fully access), to compliance (a patient who could not maintain home hygiene during the early healing window), to systemic (uncontrolled diabetes or persistent smoking). When a site does not respond, the conversation at the six-month visit is about the next step, which may include retreatment of that specific site, surgical access at that site, or a maintenance plan that monitors the area more closely.
This honesty about partial outcomes is one of the reasons measured clinical language matters more than promotional language. LANAP works well across most treated sites in most patients. It does not work equally well in every site in every patient, and that is true of every periodontal therapy ever studied. The patients who get the best long-term outcomes are the ones who go in with realistic expectations and stay engaged with the maintenance program through the years that follow.
Ready to Restore Your Gum Health?
If you have been diagnosed with moderate to advanced periodontitis and want to understand the realistic outcome curve for your specific situation, the next step is a consultation with comprehensive pocket charting, an honest discussion of your risk profile, and a transparent treatment plan. Dr. Parachuru completed his periodontics certificate at the University of Minnesota alongside a PhD in Immunology, which means LANAP candidates at Prosper Periodontics are evaluated by a specialist who understands both the laser physics and the systemic biology that shapes long-term outcomes. We see patients from Prosper, Frisco, McKinney, Celina, and Aubrey at our office at 2300 E Prosper Trail Suite #20.
To schedule, call (972) 787-1122 or request a consultation online. Learn more about the protocol on our LANAP service page, explore the comparison in our LANAP vs traditional gum surgery guide, or review week-by-week healing in our LANAP recovery timeline. Frisco-area patients can also visit our LANAP laser gum treatment in Frisco, TX page.