Stages of Periodontal Disease: From Gingivitis to Advanced

When a dental hygienist tells you that you have periodontitis, the first question worth asking is which stage. The answer changes almost everything that follows. The four stages of periodontal disease run from gingivitis (fully reversible) through advanced periodontitis (where the goal shifts to saving teeth that are already loose), and the treatment pathway, the prognosis, and the probability of keeping each tooth all depend on where you sit on that spectrum. CDC surveillance data indicates that roughly 47 percent of adults aged 30 and older in the United States have some form of periodontitis, and that figure climbs above 70 percent in adults 65 and older. This guide walks through what each stage looks like clinically, what you might notice at home, and what Dr. Praveen Parachuru evaluates during a periodontal exam at Prosper Periodontics.
What Are the Four Stages of Periodontal Disease?
Periodontal disease is staged on a continuum from gingivitis through early, moderate, and advanced periodontitis, and only the first stage is fully reversible because it has not yet damaged the bone supporting your teeth.
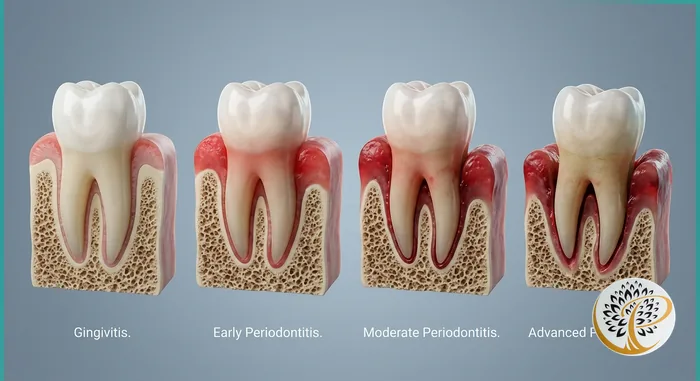
The American Academy of Periodontology and the European Federation of Periodontology issued a joint classification in 2017 that staged periodontitis using clinical attachment loss, radiographic bone loss, and tooth loss attributable to periodontitis. In day-to-day clinical language, most patients hear about four stages. Stage one is gingivitis, which is inflammation confined to the gum tissue with no attachment loss and no bone loss. Stage two is early periodontitis, where the attachment between gum and tooth has begun to break down and small amounts of bone are lost. Stage three is moderate periodontitis, with deeper pockets, visible bone loss on X-rays, and the first signs of tooth mobility in some cases. Stage four is advanced or severe periodontitis, where bone loss extends to or beyond half of the root length, multiple teeth are mobile, and tooth loss has often already occurred.
The reason staging matters is that the biology shifts as you move through the stages. In gingivitis the tissue is inflamed but the underlying bone and ligament are intact, and removing the bacterial cause allows the gums to return to a healthy state. Once attachment is lost and bone has receded, the body cannot regenerate that architecture spontaneously. Treatment becomes about halting further loss and, in select cases, attempting regeneration through specific surgical or laser-based therapies.
What Does Stage One Gingivitis Look Like?

Gingivitis is bacterial inflammation of the gum tissue without any loss of attachment or bone, and it is the only stage of periodontal disease that can be fully reversed with professional cleaning and improved home care.
The classic signs of gingivitis are red gum tissue at the margin where it meets the tooth, mild puffiness or rolled edges along the gumline, bleeding during brushing or flossing, and sometimes mild bad breath. The pockets between gum and tooth measure within the normal range of one to three millimeters when probed during a hygiene visit. There is no recession that is attributable to disease. There is no bone loss visible on X-rays. The teeth feel solid in their sockets.
What gingivitis represents is the immune system reacting to the bacterial biofilm (plaque) that accumulates along the gumline when home care is incomplete. The bacteria release endotoxins that the gum tissue interprets as a threat, and the inflammatory response brings increased blood flow, swelling, and the bleeding that patients notice when they floss. None of this has yet damaged the bone or ligament. Studies suggest that thorough professional cleaning combined with consistent twice-daily brushing and daily interdental cleaning can resolve gingivitis within two to three weeks in most patients.
The reason periodontists emphasize the gingivitis stage is that gingivitis is the warning shot. Patients who notice bleeding gums and adjust their habits avoid the cascade that leads to periodontitis. Patients who ignore the bleeding for years are the ones who eventually arrive in our office with the deeper-stage disease covered below. Our guide on the signs of gum disease covers the at-home indicators in more detail, and our guide on whether gum disease can be reversed walks through what is and is not reversible at each stage.
What Distinguishes Stage Two Early Periodontitis?
Early periodontitis is the point at which the inflammatory process has crossed from soft tissue into the underlying attachment, producing pockets of four to five millimeters and small amounts of bone loss that show on dental X-rays.
Patients with early periodontitis often feel that something has changed but cannot describe it precisely. The gums may bleed more reliably during flossing. There may be a faint metallic taste in the morning. The teeth may look slightly longer in the mirror because the gums have receded one or two millimeters. Probing depths during a periodontal exam reveal pockets in the four-to-five millimeter range, which is too deep for a toothbrush bristle to clean effectively. Bitewing or periapical X-rays start to show horizontal bone loss of one to two millimeters along the crests between teeth.
The treatment at this stage is non-surgical periodontal therapy, commonly called scaling and root planing or a deep cleaning. The hygienist or periodontist uses ultrasonic and hand instruments to remove the calcified deposits (calculus) from the root surfaces below the gumline and smooths the root so that the gum tissue can reattach. Local anesthesia is typically used because the work happens below the gumline where the tissue is sensitive. The procedure is usually completed in one or two visits depending on how many quadrants of the mouth are affected.
Outcomes at this stage are generally excellent when the patient follows through with the home care changes and the recommended maintenance schedule. Pocket depths typically reduce by one to two millimeters at the re-evaluation appointment six to eight weeks after treatment, and bleeding on probing decreases substantially. The bone loss that has already occurred does not reverse, but the active disease process is halted and the remaining bone is preserved.
What Are the Markers of Stage Three Moderate Periodontitis?
Moderate periodontitis is defined by pockets of six to seven millimeters, bone loss extending into the middle third of the root, and the first appearance of tooth mobility or bite changes that some patients begin to notice during normal chewing.
By this stage the disease has been progressing silently for years in most patients. The probing depths around several teeth measure six to seven millimeters, which means the tip of the periodontal probe is reaching the level where the bone has receded substantially below where it should sit. Radiographic bone loss is clearly visible on X-rays, often involving the area between the roots of multi-rooted teeth (called furcation involvement). Some teeth begin to show mobility when the periodontist tests them with two instrument handles. Patients sometimes notice that their bite feels slightly off, or that food packs into spaces between teeth that did not exist before.
Treatment at this stage usually requires more than scaling and root planing alone. Options include traditional periodontal flap surgery, where the gum tissue is reflected to allow direct visual access to the root surface and bone for thorough cleaning and reshaping, and laser-assisted protocols such as LANAP, which use a specific Nd:YAG laser to disinfect pockets and support regeneration without incisions. The choice between these depends on pocket depth, bone defect anatomy, medical history, and patient preference. Our LANAP versus traditional gum surgery comparison walks through the trade-offs in detail.
The prognosis at moderate stage is good for most teeth when treatment is completed and maintenance is consistent. Some teeth with severe localized bone loss may have a guarded prognosis even after successful surgery, meaning they are kept under closer observation for signs of further breakdown. Patients at this stage transition into a periodontal maintenance schedule of every three to four months rather than the standard six-month cleaning interval.
What Does Stage Four Advanced Periodontitis Involve?
Advanced periodontitis describes the point at which bone loss has reached or exceeded half the length of the tooth root, multiple teeth are mobile or have shifted, and the conversation has shifted from preserving every tooth to deciding which teeth can realistically be saved.
The clinical picture at stage four is unmistakable. Probing depths of eight millimeters or more are common. Pus may discharge from the gumline when pressure is applied. Teeth visibly shift or appear to flare outward, particularly in the upper or lower front. Severe bone loss on X-rays extends to or below the apex of the root in the worst-affected teeth. Patients describe gums that feel chronically sore, persistent bad breath that is not addressed by mouthwash, and a sense that food becomes trapped almost everywhere they chew.
Treatment planning at this stage is individualized to a degree that earlier stages are not. Some teeth are still saveable through aggressive periodontal surgery, bone grafting, and meticulous maintenance. Others have lost so much support that extraction and replacement is the more predictable path. The decision balances the cost and time investment of attempting to save a tooth against the long-term reliability of replacement options including bridges and dental implants. When extractions are necessary, immediate planning for the replacement protects the remaining bone and prevents the adjacent teeth from drifting.
Patients with advanced periodontitis benefit from being seen by a periodontist rather than a general dentist for two reasons. First, the surgical and regenerative options at this stage require specialty training. Second, the systemic implications of advanced periodontitis are not theoretical. Studies indicate that patients with severe periodontitis have measurably elevated cardiovascular and metabolic risk, and treating the periodontal infection has been shown to reduce systemic inflammatory markers. Our companion guide on the gum disease, heart disease, and diabetes connection covers this in depth.
How Does a Periodontist Determine Which Stage You Are In?
Staging requires a comprehensive periodontal exam that includes six-point pocket probing around every tooth, mobility assessment, furcation evaluation, and full-mouth radiographs that show the level of bone support around each root.
A standard hygiene visit at a general dental office often does not capture the data needed to stage periodontal disease accurately. The periodontal exam at our office begins with a medical history review that flags conditions such as diabetes, smoking history, and family history of periodontal disease. The clinical exam then measures pocket depth at six points around each tooth (mesial, mid, distal on both buccal and lingual surfaces), records bleeding on probing at each site, evaluates each tooth for mobility on a scale from zero to three, and checks for furcation involvement on multi-rooted teeth. Recession is measured separately from pocket depth so that total attachment loss can be calculated.
Radiographs are then read for bone level, with horizontal bone loss measured as a percentage of root length and vertical (angular) defects mapped to specific teeth. The combination of clinical and radiographic findings produces the stage assignment. Grade is assigned separately based on rate of progression, which considers how rapidly the disease has advanced relative to the patient’s age and risk factors.
What patients should expect from this exam is roughly forty-five to sixty minutes of focused evaluation rather than a quick look. Our first visit periodontist guide describes the appointment in more detail. The output is a written treatment plan that names the stage, identifies which teeth are at greatest risk, and lays out the recommended therapy with realistic expectations for what each step will accomplish.
Can the Damage From Earlier Stages Be Reversed?
The bone and attachment loss from periodontitis cannot be regrown spontaneously, but specific treatments including LANAP and guided tissue regeneration can produce measurable new attachment in selected defects, and the active disease process at every stage can be halted with appropriate therapy.
The honest answer here matters because patients sometimes encounter marketing language that suggests gum disease can be cured or fully reversed through home care alone or through any number of products. Once attachment loss has occurred, brushing technique cannot bring back the bone or the ligament. What good home care can do is prevent further loss, which is its own meaningful outcome.
Where regeneration is possible, it requires specific clinical conditions and specific therapies. Vertical bone defects with sufficient remaining bony walls are sometimes amenable to grafting and barrier membrane techniques. Certain laser protocols, specifically the Nd:YAG laser used in the LANAP procedure, hold FDA clearance for cementum-mediated new attachment with new bone formation. Even in these cases, regeneration is partial rather than complete, and not every site responds. The realistic outcome of well-executed periodontal therapy at any stage is stable disease, preserved teeth, and a manageable maintenance schedule for the long term.
The maintenance side of this is not optional. Periodontitis is a chronic disease in the same family as diabetes or hypertension. There is no point at which a patient is cured. The condition is managed through ongoing professional care every three to four months and consistent home care for life. Patients who understand this from the start tend to do well over decades. Patients who treat the initial therapy as a one-and-done event are the ones who return with recurrence.
Ready to Restore Your Gum Health?
If you have noticed bleeding gums, persistent bad breath, or any of the warning signs described above, the value of an early periodontal evaluation is significant regardless of which stage you turn out to be in. Dr. Praveen Parachuru completed his periodontics certificate at the University of Minnesota alongside a PhD in Immunology, which means staging and treatment planning at Prosper Periodontics is performed by a clinician who understands both the surgical management and the underlying inflammatory biology that drives periodontal disease. We see patients from Prosper, Frisco, McKinney, Celina, and Aubrey at our office at 2300 E Prosper Trail Suite #20.
To schedule an evaluation, call (972) 787-1122 or request an appointment online. You can also learn more about our complete approach on the periodontal care service page or read about the link between gum disease and systemic health to understand why early intervention matters beyond saving teeth.