Can LANAP Regrow Bone? The Science of Regeneration

Patients ask whether LANAP can actually regrow bone more often than they ask any other clinical question about the procedure. The honest answer is yes, the published histology shows that LANAP supports true periodontal regeneration including new bone, but the more useful answer requires distinguishing between regeneration and repair, between defect types that respond well and defect types that respond modestly, and between the histological evidence and the radiographic appearance most patients want to see on their next x-ray. This guide walks through the biology of bone regeneration, what the Yukna 2007 study actually demonstrated, which infrabony defects regenerate best, and how to set realistic expectations for your own case. Dr. Praveen Parachuru performs LANAP at Prosper Periodontics with explicit attention to the defect anatomy that determines regenerative potential.
What Is the Difference Between Regeneration and Repair in Periodontal Tissue?
Regeneration is the formation of new bone, new periodontal ligament, and new cementum that recreates the original architecture of the periodontium, while repair is healing by long junctional epithelium that restores function but does not restore the original tissue components.
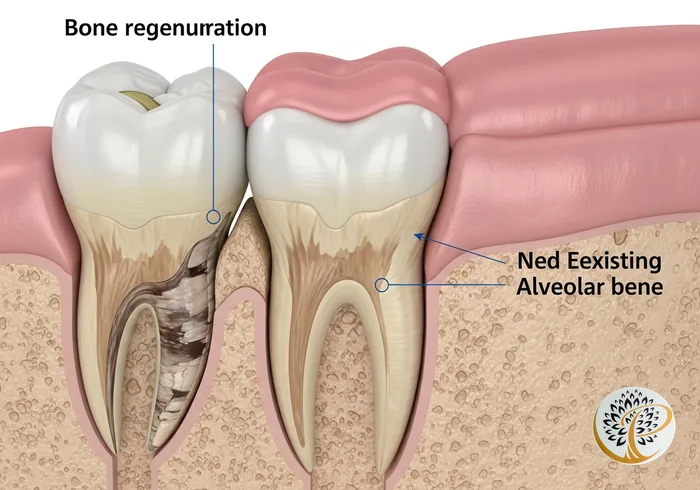
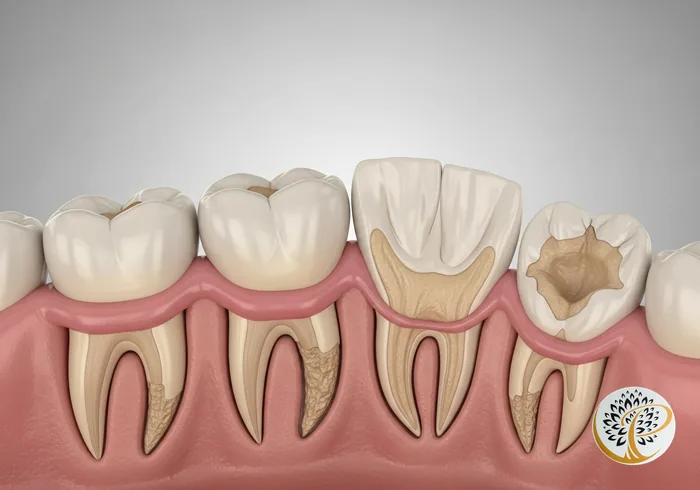
When periodontitis destroys the supporting tissues around a tooth, three components are lost: alveolar bone (the bone socket), periodontal ligament (the fibers that anchor the tooth to the bone), and cementum (the layer covering the root that those fibers insert into). After traditional periodontal therapy, the body heals the area, but the heal pattern matters.
Repair is the most common pattern. The gum tissue regrows down to the cleaned root surface and forms a long junctional epithelium, which is essentially a biological seal between gum and tooth. This seal restores function. It eliminates the deep bacterial pocket that was driving disease. It is genuinely useful and is the heal pattern that scaling and root planing and most traditional flap surgery produce. The trade-off is that the original three-component architecture is not restored. The tooth is now anchored less robustly to the surrounding bone than it was before disease.
Regeneration is the rarer and more biologically demanding outcome. Regeneration restores all three components: new bone fills in where bone was lost, new ligament fibers form, and new cementum is deposited on the previously diseased root surface so the new ligament fibers have something to insert into. The result is a tooth supported in the same architecture it had before disease. From a clinical standpoint, this is what every periodontal therapy is aiming for, but only a few therapies have produced histological evidence that they actually achieve it.
LANAP is one of those therapies. Other regenerative therapies include guided tissue regeneration (using a barrier membrane), bone grafting at specific defect sites, and biologic agents like enamel matrix derivatives. Each has its own indications, evidence base, and regulatory clearances. LANAP is the only laser-based protocol with histological evidence and FDA clearance for periodontal regeneration.
What Did the Yukna 2007 Study Actually Demonstrate About Bone Formation?
The Yukna et al. 2007 study published in the International Journal of Periodontics and Restorative Dentistry examined human teeth treated with the LANAP protocol three months prior to extraction, and the histological analysis showed new cementum, new periodontal ligament insertion, and new alveolar bone formation at the previously diseased root surfaces.
The study design is what makes the evidence persuasive. Patients enrolled had teeth with chronic periodontitis that were already scheduled for extraction as part of unrelated treatment plans, typically for orthodontic or restorative reasons. One side of selected teeth was treated with the LANAP protocol. The contralateral side was treated with scaling and root planing alone, serving as the control. After three months of healing, the teeth were extracted intact, sectioned histologically, and examined under microscopy.
The LANAP-treated sites showed what the regulatory pathway requires. New cementum was identified on root surfaces that had been previously denuded by disease. New periodontal ligament fibers were observed inserting into that new cementum. New alveolar bone formation was identified adjacent to the regenerated ligament. This is the three-component evidence of true periodontal regeneration. The SRP-treated sites, by contrast, showed long junctional epithelium consistent with repair.
What the study can claim and what it cannot is worth being precise about. It demonstrates that LANAP can produce histological regeneration in human tissue. It does not claim that every site in every patient regenerates to the same degree. The number of sites examined was modest by clinical-trial standards (the study examined a small number of patients with multiple sites each), and the magnitude of regeneration varied between sites. Subsequent histological work and longer-term clinical studies have generally supported the original findings, but evidence indicates that regeneration is variable and depends on factors including defect anatomy, patient health, and operator technique.
The study remains the foundational evidence behind LANAP’s FDA clearance for periodontal regeneration. No other laser-based therapy has produced equivalent published human histology, which is why other dental lasers are not cleared with the same regenerative language.
Which Bone Defects Respond Best to LANAP Regeneration?
Infrabony (vertical) defects with two or three remaining bony walls respond best to LANAP regeneration, while one-wall defects, severe furcation involvement, and horizontal bone loss respond more like repair than full regeneration.
The geometry of the bone defect is the strongest predictor of how much regeneration is biologically possible. Periodontitis can destroy bone in different patterns, and not all patterns are equally amenable to regrowth.
Three-wall infrabony defects are the most favorable. These are vertical defects where the bone destruction has formed a pocket bordered by remaining bone on three sides, with the tooth root forming the fourth surface. The remaining bony walls supply blood supply and progenitor cells from three directions, which means the regenerative potential is high. Pocket depths in these defects often reduce by four to six millimeters or more after LANAP, with substantial new bone fill visible on radiographs over the months that follow.
Two-wall defects are intermediate. The remaining bone supplies progenitor cells from two directions, regeneration is achievable, and clinically meaningful pocket reduction is typical. Most published LANAP outcomes are reported as averages across mixed defect types, and the better-responding two- and three-wall defects pull the averages up.
One-wall defects are less favorable for regeneration. With only one remaining bony wall, the regenerative cells have less surface area to migrate from, and the defect tends to heal more by repair than by full regeneration. Clinically meaningful improvement still occurs, but the radiographic bone fill is usually modest, and the tissue response looks more like long junctional epithelium with some bone proximity than like full reattachment.
Furcation involvement, where bone loss has reached the area between the roots of multi-rooted teeth, is a category of its own. Class I furcation (incipient bone loss) responds reasonably well. Class II (moderate) responds variably. Class III (through-and-through) is generally beyond what any periodontal regenerative therapy can fully reverse, including LANAP. These cases are evaluated individually, and Dr. Parachuru is candid when furcation severity argues for a different treatment plan.
Horizontal bone loss, in which the bone level has reduced uniformly across an arch without distinct vertical defects, is the least favorable scenario for any regenerative therapy. The remaining bone is at a lower level, and there are no walls to regenerate against. LANAP in these cases improves pocket depth and tissue health but does not produce significant vertical bone gain.
How Long Does Bone Regeneration Take After LANAP?
Bone regeneration after LANAP is a months-to-years process. The early fibrin scaffold forms in days, soft-tissue reattachment happens over weeks, initial bone fill becomes radiographically visible at three to six months, and remodeling continues for twelve to twenty-four months.
The biology unfolds in stages. The day of the procedure, the laser creates a stable fibrin clot at the base of each treated pocket. This clot is the biological scaffold for what comes next. It seals the pocket against bacterial recolonization and provides a matrix for cells to migrate into.
Over the first one to three weeks, soft tissue reattachment begins. New connective tissue grows against the cleaned root surface. Inflammation resolves. Pocket depths begin to measure shallower as soon as the treated tissue tightens against the tooth.
Over the first three to six months, the more demanding regenerative biology happens. Progenitor cells migrate from the periodontal ligament space and the surrounding bone into the defect. New cementum is deposited on the root. New ligament fibers form and orient themselves to insert into the new cementum. New bone forms along the previously diseased socket. By the six-month re-evaluation, both clinical pocket depth measurements and radiographic bone fill typically show meaningful improvement.
Over the next six to eighteen months, remodeling continues. Bone density at the regenerated sites increases. Tissue maturation proceeds. Patients who attend their three- or four-month maintenance visits during this window allow the periodontist to monitor the response and address any sites that are not progressing as expected.
The patience aspect of this timeline matters for setting realistic expectations. Patients who expect their next post-treatment x-ray to look dramatically different may be disappointed; the radiographic changes appear gradually over months, not weeks. The functional improvement (less bleeding, less inflammation, no progressive loosening) is usually felt before the radiographic change is visible.
Why Do Some Sites Regenerate While Others Just Repair?
The combination of defect anatomy, blood supply, root surface condition, patient systemic health, and operator technique determines how each individual treated site responds. Even within the same patient and the same treatment session, some sites can show full regeneration while others heal more by repair.
This variability is one of the more honest aspects of regenerative periodontics that marketing materials sometimes elide. Studies show that average responses across patient populations are encouraging, but individual sites within a single mouth respond differently. Understanding why helps set expectations.
Defect anatomy is the strongest single factor, as discussed above. Three-wall and two-wall infrabony defects regenerate well. One-wall defects and broad horizontal loss regenerate modestly.
Blood supply is the next factor. Sites with robust vascular supply heal more completely. Sites in areas of compromised blood flow (heavy smokers, severe vascular disease, prior radiation therapy to the head and neck) heal less completely. Smoking is the most common modifiable factor here, and patients who quit before and during treatment substantially close the gap with non-smokers.
Root surface condition matters because regeneration requires the new cementum to deposit on a clean root. Roots with deep biofilm contamination, roots with overhanging restorations that the laser cannot fully access, and roots with cervical decay or grooves all respond less consistently. Adequate root debridement during the LANAP protocol is part of why provider technique matters.
Systemic health affects the cellular work the body has to do during regeneration. Diabetic patients with elevated HbA1c, patients on systemic corticosteroids, and patients with autoimmune conditions affecting tissue healing may experience reduced regenerative response. The general health context is part of what is reviewed at the LANAP consultation.
Operator technique is the variable patients have least visibility into but is genuinely important. Standardized LANAP protocols specify laser settings, pulse durations, and treatment sequence at each step. Certified operators using the PerioLase MVP-7 with the official protocol produce more consistent regenerative outcomes than non-standardized “laser gum treatment” with other equipment. The certification matters.
How Will You Know If Bone Has Regenerated in Your Case?
Three measurements together indicate whether regeneration has occurred at your treated sites: probing pocket depth at the six-month re-evaluation, radiographic bone fill on follow-up x-rays at six to twelve months, and clinical attachment level measured at the cementoenamel junction.
Probing pocket depth is the simplest measurement. A pocket that was eight millimeters before treatment and measures four millimeters at six months has reduced by four millimeters. Some of that reduction reflects tissue tightening as inflammation resolves; some reflects actual reattachment of tissue to the root. The pocket reduction by itself does not distinguish between repair and regeneration, but a substantial reduction is a positive sign.
Clinical attachment level (CAL) is the more meaningful measurement because it accounts for the position of the gumline. CAL is measured from a fixed point on the tooth (the cementoenamel junction) to the depth of the pocket. Reduction in CAL means the tissue has actually reattached at a more coronal level, which is a stronger signal of regeneration than pocket reduction alone.
Radiographic bone fill is the visible evidence patients usually want to see. Follow-up x-rays at six and twelve months can show new bone fill at previously deep infrabony defects, particularly in two- and three-wall defects. The radiographic appearance of regeneration is sometimes subtle (a slight increase in bone density and a fill of the previously visible vertical defect), and sometimes dramatic. Either way, the comparison to pre-treatment radiographs is the visual evidence of what has happened.
The honest framing is that not every patient sees dramatic radiographic regeneration, even in successful cases. Pocket reduction, CAL gain, and reduction in bleeding on probing are usually present in successful cases. Visible radiographic bone fill is more variable. Both outcomes are clinically meaningful and contribute to long-term tooth retention.
What Does the Maintenance Look Like to Protect Regenerated Bone?
Regenerated bone is biologically real but is no more resistant to future periodontitis than the original bone was. Long-term maintenance with three- or four-month periodontal cleaning visits in the first year or two, transitioning to six-month intervals as stability is confirmed, is what protects the regenerative gains over the years that follow.
This point is sometimes missed. Bone that has regenerated after LANAP is genuine bone, integrated into the surrounding alveolar architecture. It can also be lost again if the disease that caused the original loss is not controlled. Maintenance is the continuous management of the conditions that allow the periodontal environment to stay stable.
The maintenance protocol after LANAP includes several components. Regular periodontal cleaning visits remove the biofilm and calculus that accumulate between visits. Pocket charting at each visit detects early signs of progression. Bleeding-on-probing scoring identifies sites that have become inflamed. Radiographs at intervals (typically annually or biannually) monitor bone levels. Hygiene reinforcement at each visit addresses any home-care gaps.
The risk factors that drove the original disease (smoking, uncontrolled diabetes, poor home hygiene, untreated bruxism) need to remain managed long-term. Patients who quit smoking before LANAP and then resume smoking afterward face elevated recurrence risk. Patients who were diabetic-controlled before LANAP and become uncontrolled afterward face the same elevated risk. The LANAP procedure stabilizes the disease at one moment in time. Maintenance and risk-factor management is what keeps the disease stable across the years that follow.
For broader context on what is and is not reversible across the spectrum of periodontal disease severity, our companion guide on whether gum disease can be reversed walks through the biology. The early-warning signs to watch for at home are covered in our signs of gum disease post.
Ready to Restore Your Gum Health?
If you have been diagnosed with periodontitis and want to understand the regenerative potential of LANAP for your specific defect anatomy and health profile, the next step is a consultation that includes pocket charting, radiographic evaluation of bone defects, and a candid discussion of which sites are likely to regenerate well versus heal more by repair. Dr. Parachuru completed his periodontics certificate at the University of Minnesota alongside a PhD in Immunology, which means LANAP candidates at Prosper Periodontics are evaluated by a clinician who understands both the laser physics and the cellular biology of periodontal regeneration. We see patients from Prosper, Frisco, McKinney, Celina, and Aubrey at our office at 2300 E Prosper Trail Suite #20.
To schedule, call (972) 787-1122 or request a consultation online. Learn more about the protocol on our LANAP service page, compare procedural options in our LANAP vs traditional gum surgery guide, or review week-by-week healing in our LANAP recovery timeline. Frisco-area patients can also visit our LANAP laser gum treatment in Frisco, TX page.