Periodontal Maintenance vs Regular Cleaning: What’s Different

Patients diagnosed with periodontitis are often told at the end of their initial therapy that future cleanings will be different. The schedule shifts from twice a year to every three or four months, the appointment runs longer, the insurance code changes, and the out-of-pocket cost frequently rises. None of this is optional. Periodontal maintenance is a different procedure from a regular cleaning, performed for a different reason, and it continues for life because periodontitis is a chronic condition that is managed rather than cured. This guide walks through the clinical, billing, and long-term differences so patients understand what they are paying for and why Dr. Praveen Parachuru and the team at Prosper Periodontics structure care this way.
What Is the Clinical Difference Between a Regular Cleaning and Periodontal Maintenance?

A regular cleaning (prophylaxis, dental code D1110) addresses plaque and tartar above the gumline on patients with healthy gums, while periodontal maintenance (D4910) cleans both above and below the gumline on patients with a documented history of periodontitis and includes ongoing management of the deeper sites that supported the original disease.
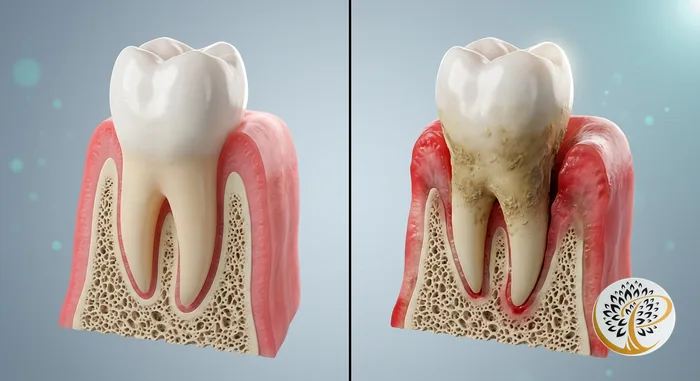
A prophylaxis is built around a healthy mouth. The hygienist removes soft plaque and calcified deposits (calculus) along the gumline and on the visible portions of the tooth, then polishes the surfaces. Probing depths measure within the normal one to three millimeters with no attachment loss and no bleeding pattern that suggests active disease. The procedure is preventive in the strict sense of the word.
Periodontal maintenance is structured for a mouth that has crossed into disease and been brought back to a stable state through scaling and root planing or periodontal surgery. The hygienist or periodontist performs the supragingival cleaning a prophylaxis includes and continues into the deeper sites. Subgingival scaling removes the calculus and biofilm that accumulate below the gumline within residual pockets, root surfaces are reinstrumented where needed, pocket depths are remeasured at each visit, and bleeding on probing is mapped to identify recurrence early.
A prophylaxis is typically scheduled for thirty to forty-five minutes. A periodontal maintenance visit runs sixty minutes or longer because the subgingival work and reassessment require time a healthy mouth does not need.
Why Does the Frequency Change From Six Months to Three or Four Months?
The three-to-four-month interval reflects the time it takes for the bacteria responsible for periodontitis to recolonize subgingival sites and reach population densities that can restart the destructive process, and shorter intervals are therefore protective in a way that the standard six-month interval is not.
Periodontal pathogens such as Porphyromonas gingivalis, Tannerella forsythia, and Treponema denticola form biofilms within gum pockets that are not fully removed by even diligent home care. Studies suggest that by twelve to sixteen weeks after a thorough subgingival cleaning, the bacterial load returns to levels capable of triggering renewed attachment loss. Cleaning every three to four months interrupts that cycle before destructive thresholds are reached.
The six-month interval was developed for prevention of caries and gingivitis in patients who do not have periodontitis. It is too long for periodontitis patients because the recolonization timeline outpaces the recall. Patients sometimes ask whether they can return to a six-month schedule after years of stable maintenance. The honest answer is that the underlying susceptibility does not change. The immune profile, bacterial flora, and anatomical factors that made the patient susceptible are still present, and stretching the interval has been associated in the literature with increased recurrence.
Why Does Insurance Often Push Back on the Coding Change From D1110 to D4910?
Dental insurance plans reimburse prophylaxis (D1110) and periodontal maintenance (D4910) at different rates and frequency limits, and the coding shift can trigger benefit limitations, alternate benefit substitutions, or outright denials that surprise patients who were not aware of how the codes are treated.
D1110 and D4910 are mutually exclusive within an episode of care. Many plans cover two D1110 cleanings per calendar year at a high reimbursement rate (often 80 to 100 percent in network). When a patient transitions to D4910, several things can happen depending on plan language. Some plans cover D4910 at the same frequency and rate as D1110. Others cover four D4910 visits a year matching the recommended interval. Others reimburse D4910 at a reduced percentage, producing a higher copay even though the procedure cost is greater. Others apply an alternate benefit clause and reimburse only the equivalent of two D1110 procedures per year, leaving the patient responsible for the difference on additional visits.
Plan limitations sometimes require that scaling and root planing (D4341 or D4342) appear in the patient’s recent history before D4910 is reimbursed, which verifies the periodontitis diagnosis. The documentation requirement is straightforward when treatment was rendered in the same office and can become a barrier when patients change practices. Our office verifies benefits before each visit and provides a written estimate. For patients with restrictive benefits, Cherry financing offers a way to spread maintenance costs without surprises.
Why See a Periodontist for Maintenance Rather Than a General Dentist?
Periodontal maintenance after specialty therapy is most predictably performed by the team that diagnosed and treated the original disease because the residual pocket map, the regenerative areas, and the response patterns of each site are documented in detail and the follow-up instrumentation is calibrated to that specific case.
A general dentist’s hygiene team is well-equipped to perform prophylaxis and the maintenance of straightforward cases. The question for patients with moderate or advanced periodontitis is whether the maintenance program addresses their specific residual anatomy. Periodontitis treatment leaves a map. The patient who underwent scaling and root planing in all four quadrants has different residual pocket depths than the patient who underwent osseous surgery on the upper right and laser therapy on the lower left. Maintenance instrumentation should match that map, with focused attention on the sites that were treated and the defects that were grafted or regenerated.
Periodontists also keep charting on a more detailed schedule. Comprehensive six-point probing is repeated annually at minimum, with focused probing of suspicious sites at each visit, and mobility, furcation involvement, and recession are reassessed. The data accumulates over years to show which sites are stable and which need further intervention.
Recurrence is also detected earlier in a periodontal practice. The hygienist is trained to recognize the small changes that signal active disease (a one-millimeter pocket increase, new bleeding at a stable site) and flag them at the same visit. When recurrence is caught at the four-millimeter stage, retreatment is straightforward. When missed until the seven-millimeter stage, the conversation shifts to surgery again. Our first visit periodontist guide describes the protocol, and the discussion of whether gum disease can be reversed covers what reversibility looks like at each level of severity.
Is Periodontitis Cured After the Initial Treatment?
Periodontitis is a chronic inflammatory disease that is managed rather than cured, which means a patient who has been diagnosed with periodontitis remains a periodontitis patient for life regardless of how well the initial treatment worked or how stable the disease has been since.
The phrase periodontists use is that once a patient has periodontitis, they are always a periodontitis patient. The immune response that drove the original tissue destruction is part of how that patient’s body reacts to subgingival bacteria. The bacterial flora can be reduced and disrupted but does not return to a periodontally innocent state, and the anatomical changes that occurred during the disease leave the patient predisposed to recurrence at any site that was previously affected.
Patients sometimes interpret the success of initial therapy as a return to baseline. Pockets reduced from seven millimeters to three, bleeding stopped, the instinct is to view the work as finished. The reality is that the maintenance phase is what keeps those numbers stable. Periodontitis sits in the same category as diabetes or hypertension. None is cured. Each is managed through ongoing care, and our discussion of the gum disease, heart disease, and diabetes connection covers why this matters beyond the mouth.
What Happens When Periodontitis Patients Skip Maintenance?
Patients who fall out of the three-to-four-month maintenance schedule after periodontal therapy show measurably higher rates of disease recurrence and tooth loss than patients who maintain the schedule, and the recurrence pattern is often more aggressive than the original disease because the previously affected sites are already compromised.
Long-term follow-up studies of treated periodontitis patients have repeatedly shown the same pattern. Patients who attend maintenance regularly retain the majority of their teeth at ten, fifteen, and twenty years post-treatment. Patients who lapse lose teeth at significantly higher rates and require retreatment more often.
Recurrent disease tends to be aggressive because the previously affected sites are not starting from a healthy baseline. The bone topography is already altered, and the bacterial flora has the genetic memory of having colonized those sites successfully. When maintenance is interrupted long enough for biofilm to redevelop, disease often progresses faster than in a previously healthy mouth. Pocket depths that were three to four millimeters at the last visit return to six or seven millimeters within two to three years, new mobility appears on stable teeth, and bone loss is visible on radiographs. The retreatment plan is sometimes more involved than the original treatment because recurrent disease tends to affect multiple sites simultaneously.
What Does Periodontal Maintenance Cost Over a Lifetime?
Periodontal maintenance visits typically cost in the range of two hundred fifty to three hundred fifty dollars per visit before insurance, performed three to four times per year for the patient’s lifetime, which translates to a multi-decade investment that nonetheless costs substantially less than the alternative of recurrent disease and tooth replacement.
Insurance modifies the out-of-pocket figure depending on plan benefits, deductibles, and annual maximums. Most patients with reasonable coverage pay between one hundred and two hundred dollars per visit after benefits. Across three or four visits per year, the annual cost lands between four hundred and fourteen hundred dollars before insurance. Across a thirty-year horizon (a reasonable expectation for a patient diagnosed in their forties or fifties), the total can reach into the tens of thousands of dollars.
The comparison that makes that investment worthwhile is the cost of the alternative. A single dental implant to replace a lost tooth costs three to six thousand dollars. A bone graft to rebuild a deficient ridge before implant placement adds further cost, and multiple lost teeth in a quadrant compound the figures rapidly. Patients who maintain periodontal health over decades and retain their natural teeth spend significantly less than patients whose disease recurred and required restorative reconstruction. Patients in surrounding cities can reach our team through the Frisco periodontal care page, the McKinney periodontal care page, or the Celina periodontal care page for area-specific scheduling.
When Does a Patient Transition From Regular Cleaning to Periodontal Maintenance?
A patient transitions from D1110 prophylaxis to D4910 periodontal maintenance after the diagnosis of periodontitis is established and the initial therapy (scaling and root planing or periodontal surgery) has been completed and re-evaluated, with the maintenance phase typically starting six to eight weeks after the conclusion of active treatment.
A comprehensive periodontal exam stages the disease and identifies the appropriate initial therapy. Stage one gingivitis typically responds to thorough cleaning and improved home care without crossing into the maintenance category. Stage two early periodontitis is usually managed through scaling and root planing in two to four quadrants, with re-evaluation six to eight weeks later. Stage three moderate periodontitis often requires scaling and root planing followed by surgical or laser-based therapy at sites that did not respond adequately. Stage four advanced periodontitis usually requires more extensive surgical treatment and sometimes targeted extractions.
Once initial therapy is complete and re-evaluation confirms active disease has been controlled, the patient transitions into maintenance. The first maintenance visit is scheduled three to four months after re-evaluation, and the coding shifts from D1110 to D4910 at that point.
For patients who have undergone laser-based regenerative therapy, the maintenance phase has additional considerations. Sites where regeneration was attempted are monitored for evidence of new attachment formation, and instrumentation in those areas is performed cautiously to avoid disrupting healing tissue. Our LANAP versus traditional gum surgery comparison and the LANAP recovery timeline cover what regenerative cases look like and how that affects maintenance instrumentation in the months after surgery.
Ready to Restore Your Gum Health?
If you have been diagnosed with periodontitis and are uncertain whether your current cleaning schedule reflects your condition, an evaluation can confirm that the maintenance program matches the disease history. Dr. Praveen Parachuru completed his periodontics certificate at the University of Minnesota alongside a PhD in Immunology, so maintenance protocols at Prosper Periodontics are calibrated by a clinician who understands both the surgical management and the inflammatory biology that determines long-term stability. We see patients from Prosper, Frisco, McKinney, Celina, and Aubrey at our office at 2300 E Prosper Trail Suite #20.
To schedule a maintenance evaluation or transfer your care to our practice, call (972) 787-1122 or request an appointment online. Learn more on the periodontal care service page or read about our laser-based periodontal therapy for patients whose disease history involved regenerative treatment.